Your patient is anemic. That's the easy part. Now figure out why.
Microcytic - Macrocytic / Normocytic - Hemolytic - IDA workup
If you get one wrong, it bounces back - try again.
Most common anemia worldwide. The body doesn't have enough iron to make hemoglobin, so the cells come out small and pale.
Blur → reveal → next beat.



Each anemia type is a villain with a different weapon. The lab signature sits directly under the story so the discriminator cannot hide.
The empty warehouse. Body is out of iron. Cells come out thin and pale.
The genetic imposter. Looks like IDA but iron studies are completely normal.
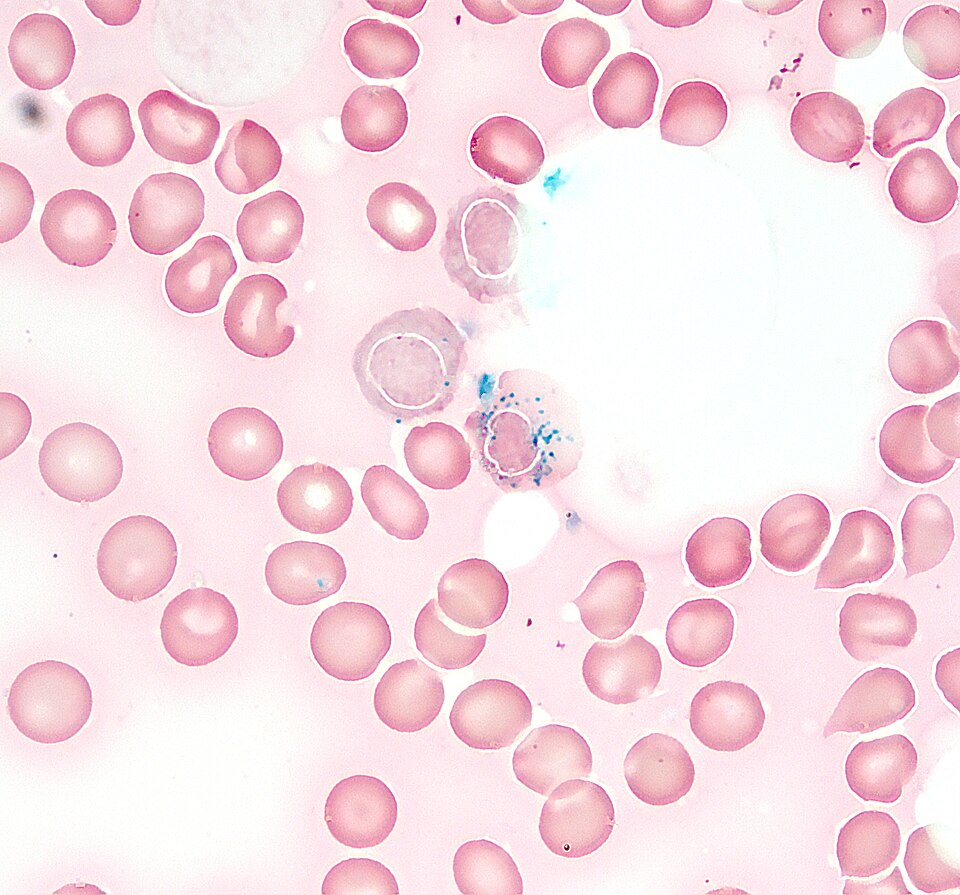
The hoarder. Has iron but can't use it. Iron piles up in the mitochondria.
The saboteur. Body hides iron on purpose via hepcidin. Has iron. Won't share it.
The neurologist's nightmare. Big cells AND neuro damage. The only one that hurts your spine.
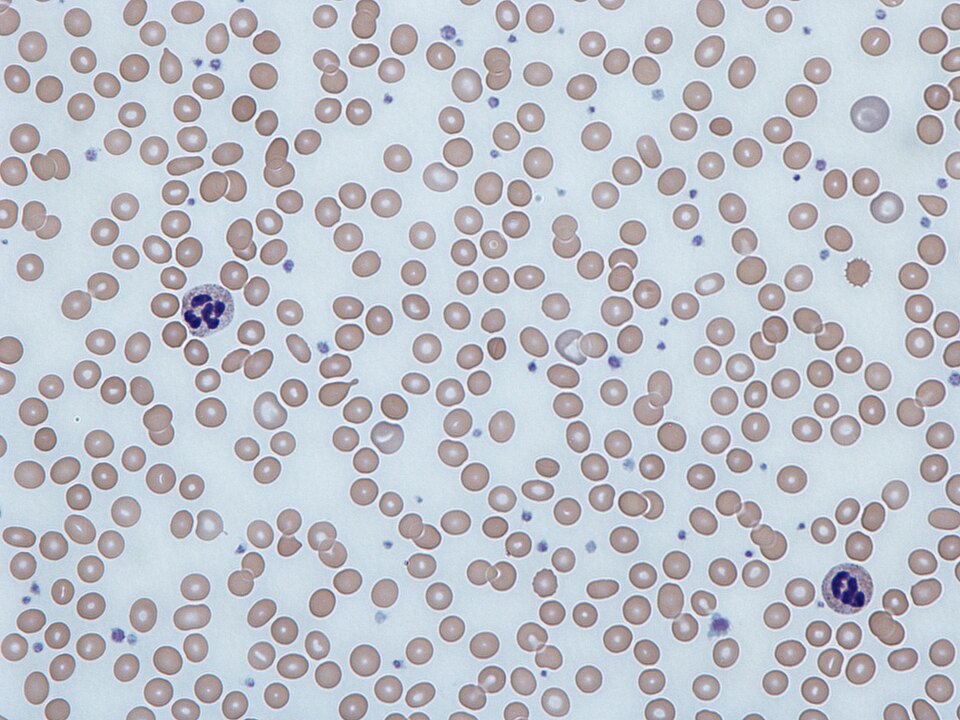
The destroyer. Cells are made fine but burst before their time. Marrow can't keep up.
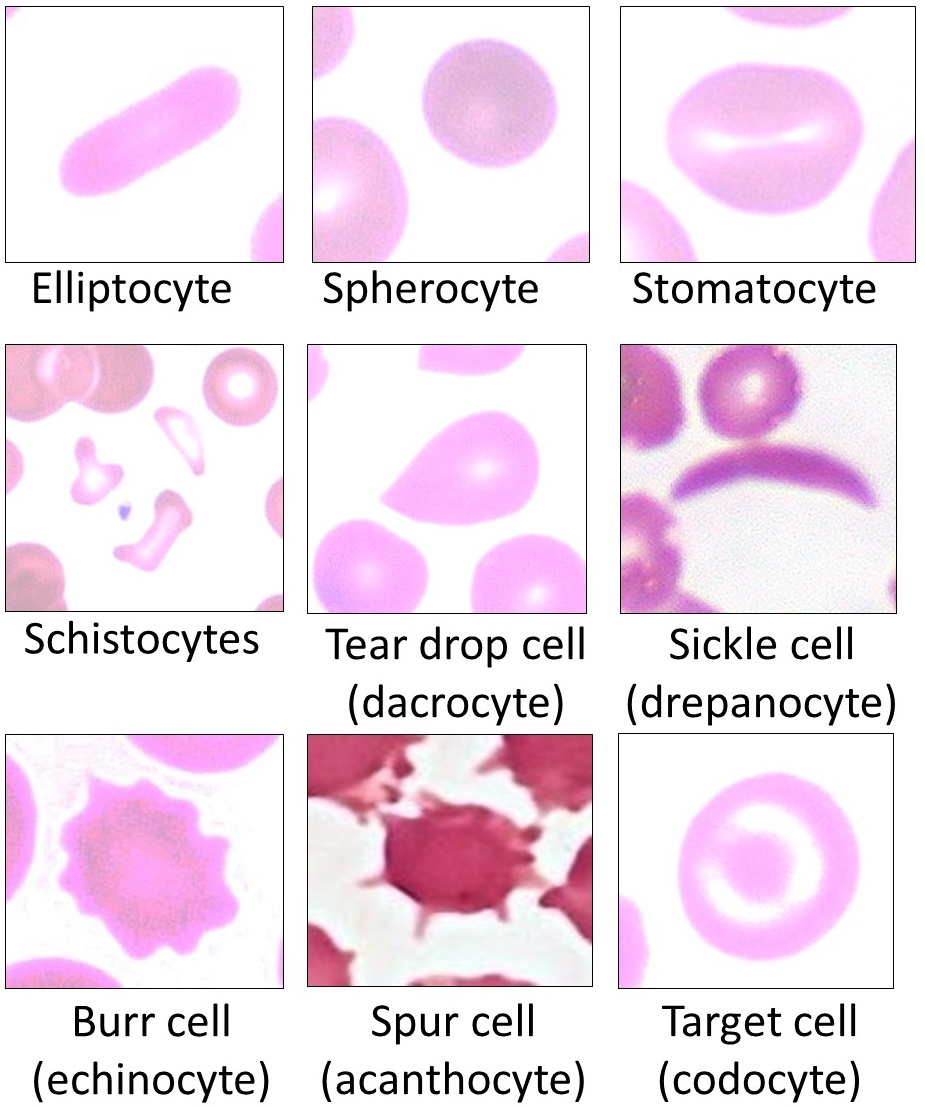
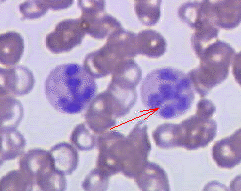
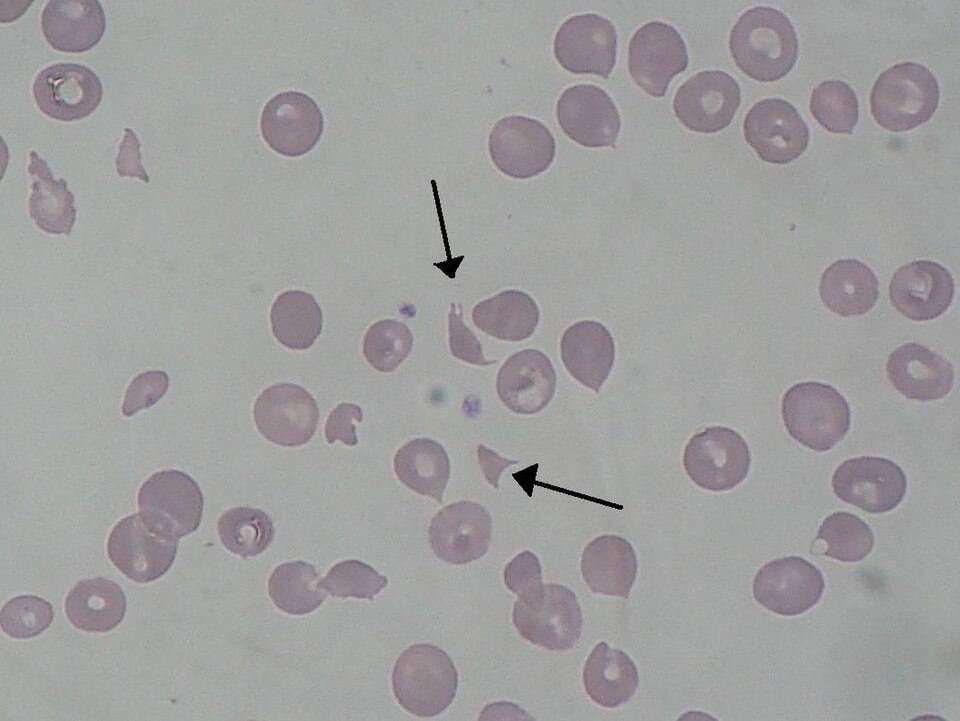
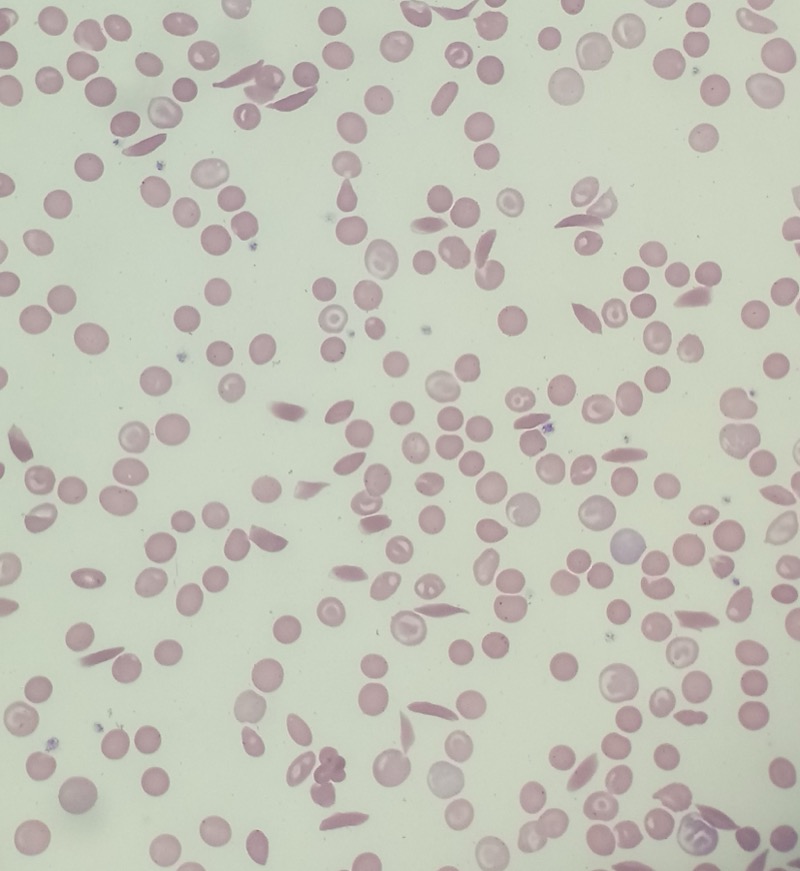
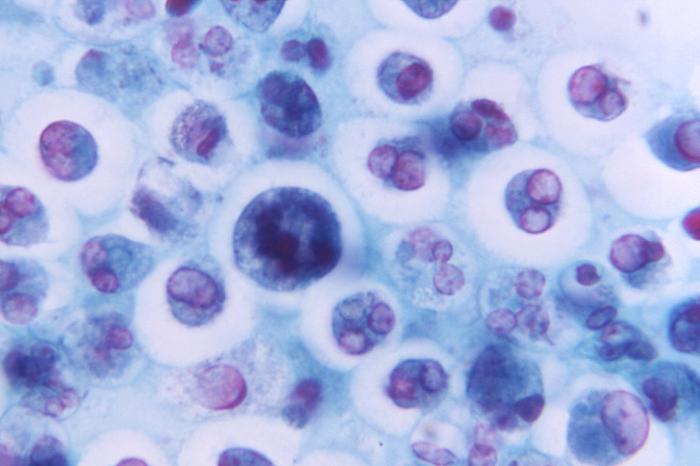
Free-use morphology anchors for the diseases above. Tap any image to expand.

Hemolytic Anemia Lab Logic
Every red cell that dies gets taken apart. Hemoglobin breaks down into heme, and heme becomes bilirubin. The indirect form is the raw, freshly made version before the liver conjugates it. When cells die faster than the liver can process them, indirect bilirubin backs up in the blood. Enough backup and the patient turns yellow. The liver is not failing. It is buried under the load.
Haptoglobin is a blood protein whose entire job is to grab free hemoglobin that spills out when red cells burst. Think of it as the cleanup crew. When a lot of cells burst fast, free hemoglobin floods the plasma, and haptoglobin binds it until the supply runs out. Empty crew = it was all used up = active hemolysis. Low haptoglobin is one of the most specific signs of hemolysis.
Megaloblastic anemia + neurological symptoms. B12 is needed for DNA synthesis AND myelin maintenance.
Same megaloblastic picture as B12 - hypersegmented neutrophils, macro-ovalocytes. But NO neuro symptoms.
Big cells but NO hypersegmented neutrophils. DNA synthesis is fine - the cell membrane is just weird.
MCV is normal. The cells are the right size - there just aren't enough of them, or they're being destroyed. Split by reticulocyte count.
Red cells are being destroyed before their 120-day lifespan. The marrow tries to compensate → ↑ reticulocytes.
| Iron Deficiency | Chronic Disease | |
|---|---|---|
| Ferritin | ↓↓↓ (empty) | ↑ (trapped) |
| TIBC | ↑ (hungry) | ↓ (not looking) |
| Serum iron | ↓ | ↓ |
| % Sat | ↓ | ↓ |
Both have low serum iron. The split is ferritin (empty vs full warehouse) and TIBC (desperate vs indifferent).
Patient is anemic. Walk through the decision tree. I'll quiz you at each branch.
Use the CBC like a routing console: size the red cells first, then order the lab that actually separates the bucket.
Small cells usually mean heme or globin production failed. Ferritin and TIBC decide whether iron is missing, trapped, or not the problem.
The cells are normal-sized. The key is whether the marrow is trying hard enough to replace what is missing.
Large cells need a DNA-synthesis check first. Hypersegmented neutrophils push you toward B12 and folate.
clinical vignettes. One at a time. Cross out wrong answers, highlight the clue. Reveal the chain.
The active board walkthrough lives in the main Board Walkthrough section.
{kind=link}