The single most impactful lifestyle change you can prescribe for any smoker with established disease
Before we start
A 63-year-old man with a 40 pack-year history is newly diagnosed with heart failure (EF 30%). His cardiologist adds lisinopril, carvedilol, and furosemide. You are his primary care physician at follow-up. What is the single most important lifestyle change to recommend?
From the Attending
The exam loves this question. The distractor list is always convincing: daily walks, reducing red meat, cutting sodium, meditating. All fine. None of them move the mortality needle the way stopping tobacco does in a smoker with heart failure, COPD, or vascular disease. If the patient smokes, that is the answer. Every time.
Students second-guess this answer because diet and exercise are also modifiable. They are. But in a current smoker with established cardiovascular or pulmonary disease, no lifestyle change has the mortality data that cessation does.
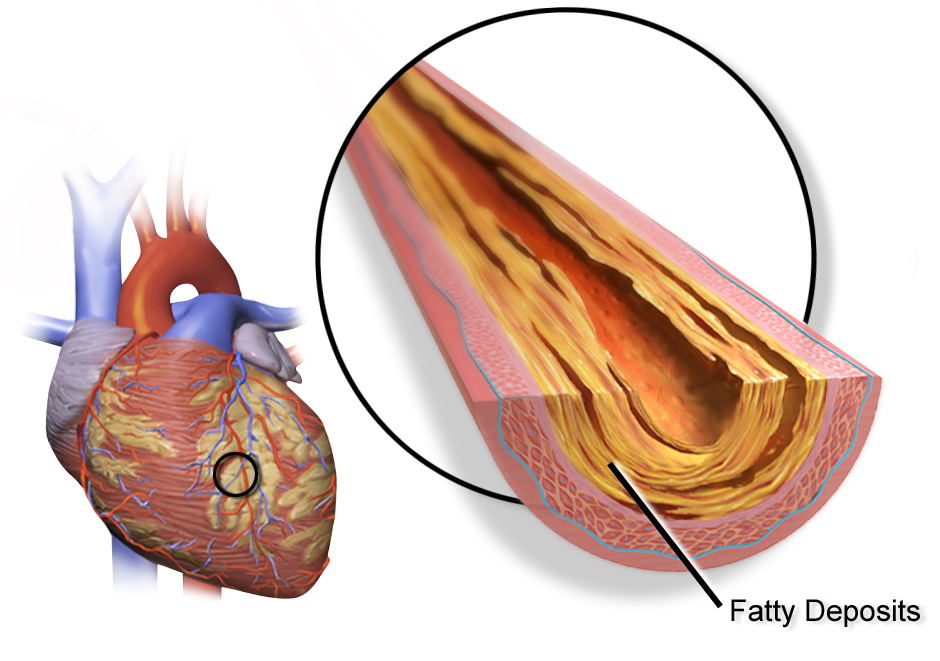
Smoking directly accelerates atherosclerosis, endothelial dysfunction, and myocardial remodeling.
In COPD: cessation is the only intervention proven to slow FEV1 decline. Bronchodilators manage symptoms. Only cessation changes the disease trajectory.
In vascular disease: cessation reduces MI risk within weeks. Diet and exercise modify risk over months to years.
In heart failure: continued smoking accelerates adverse remodeling independent of all other variables.
Coronary atherosclerosis: smoking accelerates this
1 / 7
The Framework
The 5 A's
Tap each letter to reveal what it means and the board trap inside it.
A
Ask
A
Advise
A
Assess
A
Assist
A
Arrange
Ask about tobacco use at EVERY visit. Not just new patient visits. Not just pulmonology. Every patient, every time. The exam tests whether you screen universally or only when "it seems relevant."
Advise all smokers to quit in a clear, strong, and personalized way. This is not optional for patients who are not ready. You still advise. Neutral "what do you think about smoking" framing does not count as advice.
Assess willingness to make a quit attempt in the next 30 days. This is where the path branches: if ready, move to Assist. If not ready, motivational counseling. The exam tests that Assess comes BEFORE Assist.
Assist with a quit plan: set a quit date, prescribe pharmacotherapy, provide behavioral counseling. Pharmacotherapy triples the success rate versus willpower alone. Counseling plus pharmacotherapy beats either alone.
Arrange follow-up contact within the first week after the quit date. The exam trap: students think Arrange means referral or hospitalization. It means you schedule a follow-up call or visit. The first week is the highest-relapse window.
From the Attending
The 5 A's sequence matters. Students want to jump straight to pharmacotherapy when the patient says they want to quit. But the framework is a sequence: you Ask (screen), Advise (even if they do not want to hear it), Assess (are they ready?), Assist (quit plan), Arrange (follow-up). The exam tests the ORDER. If a patient says they are motivated, the next step is Assist, not Arrange. Know your sequence.
2 / 7
The Drugs
First-Line Pharmacotherapy
Varenicline is the most effective single agent. Bupropion and NRT are alternatives and additive when combined.
Varenicline
Bupropion
NRT
MOA
Partial nicotinic agonist at alpha-4-beta-2 receptor. Gives partial stimulation (reduces withdrawal) AND blocks full nicotine binding (reduces reward).
Norepinephrine-dopamine reuptake inhibitor. Reduces craving by modulating the reward pathway. Also treats depression.
Nicotine replacement via patch (continuous), gum, lozenge, inhaler, or nasal spray (PRN). Satiates receptors without combustion products. Tapered over 8-12 weeks.
Efficacy
Highest single agent (OR ~3x vs placebo)
~2x vs placebo
~2x vs placebo. Combining patch + short-acting form improves rates further.
Contraindicated
Caution in serious psychiatric illness. Black box warning was REMOVED (2016 EAGLES trial). NOT contraindicated by seizure disorder.
Severe CV disease (relative). No absolute contraindication for gum or lozenge. Safe in pregnancy (NRT is the only pharmacotherapy option in pregnancy).
Key Side Effects
Nausea (take with food), vivid dreams, sleep disturbance
Dry mouth, insomnia, headache, seizure risk at high doses
Anorexia nervosa or bulimia nervosa (electrolyte imbalance from purging + bupropion = catastrophic seizure risk)
Concurrent MAO inhibitor use (14-day washout required)
Abrupt alcohol or benzodiazepine withdrawal (already lowers seizure threshold independently)
From the Attending
The big trap on varenicline: the FDA removed the black box warning for psychiatric events in 2016 after the EAGLES trial showed no increased risk of neuropsychiatric adverse events compared to placebo. Students who memorized the old black box get this wrong. Know the update.
And know the bupropion contraindication cold. Eating disorder plus bupropion equals seizure. The mechanism: purging causes hypokalemia and hypomagnesemia, both of which independently lower the seizure threshold. Bupropion stacks on top. This is an absolute contraindication even in remission.
3 / 7
Quantifying Exposure
Pack-Years, Screening, and the COPD Connection
Pack-years = (packs per day) x (years smoked). One pack = 20 cigarettes. This is the exposure unit for lung cancer screening.
20 pack-years
Lung cancer screening threshold: age 50-80 with ≥20 pack-years (USPSTF 2021). Annual low-dose CT.
From the Attending
The USPSTF updated in 2021: 20 pack-years (not 30), starting at age 50 (not 55). Three criteria must ALL be met: age 50-80, at least 20 pack-years, and current smoker OR quit within the last 15 years. If a patient is 50, smoked 1 pack/day for 20 years, and quit within the last 15 years, they qualify for annual LDCT. Know the cut-offs cold.
The COPD Connection
Smoking cessation is the only intervention proven to slow FEV1 decline in COPD. This is the single most tested fact about cessation in pulmonology.
Active smokers with COPD lose FEV1 at 80-120 mL/year.
After cessation, the decline slows to approximately 20-30 mL/year, which is the normal aging rate.
The emphysematous destruction is permanent. The alveolar surface area does not regenerate.
But the trajectory changes. The disease the patient has today is the worst it will get if they quit now.
No bronchodilator, no inhaled corticosteroid, and no supplemental oxygen changes the slope of FEV1 decline. Only cessation does.
From the Attending
The Fletcher-Peto curve tells the whole story. Three lines: non-smokers decline slowly, active smokers plummet, and quitters fall back to the non-smoker slope. The student who can draw that curve can answer any COPD cessation question on the exam. The answer is always slope change, not reversal.
4 / 7
Behavior Change
Stages of Change and Motivational Interviewing
Tap each stage to see what the patient looks like and what YOUR job is at that stage.
1
Precontemplation
2
Contemplation
3
Preparation
4
Action
5
Maintenance
Precontemplation: The patient has no intention of quitting in the next 6 months. They may not even see it as a problem. Your job: Do NOT push pharmacotherapy or quit dates. Use the 5 A's through Assess. If they are not ready, provide motivational counseling. Plant the seed. Express concern. Ask permission to discuss again at the next visit. This is where motivational interviewing lives.
Contemplation: The patient is thinking about quitting in the next 6 months but has not committed. They are ambivalent. Your job: Tip the scale. Explore ambivalence. Ask them to list their reasons to quit. Validate their concerns about quitting (weight gain, stress). Do not lecture. Motivational interviewing: open-ended questions, reflective listening, affirm their autonomy.
Preparation: The patient plans to quit within the next 30 days and has already taken steps (bought a quit date planner, told family, started reducing). Your job: This is where you Assist. Set a firm quit date. Start pharmacotherapy 1-2 weeks before the quit date (varenicline titration starts before cessation). Arrange follow-up.
Action: The patient has quit within the last 6 months. They are actively abstinent. Your job: Maintain pharmacotherapy. Address withdrawal symptoms and triggers. Arrange regular follow-up. The first week is the highest-risk relapse window. Normalize slips. The average smoker makes 8-11 attempts before sustained abstinence.
Maintenance: The patient has been abstinent for more than 6 months. Your job: Reinforce. Screen for relapse triggers (stress, social situations, weight gain). Remind them that relapse is possible even years later. Continue to Ask about tobacco use at every visit because maintenance is not permanent immunity.
Motivational Interviewing
Motivational interviewing (MI) is the evidence-based counseling approach for patients in precontemplation and contemplation. Four core principles:
Express empathy through reflective listening. Not "you should quit." Instead: "It sounds like you have been thinking about what smoking is doing to your lungs."
Develop discrepancy between current behavior and personal goals. "You mentioned wanting to be around for your grandchildren. How does smoking fit with that?"
Roll with resistance. Do not argue. If the patient pushes back, reflect it. "You are not ready right now, and that is okay. When you are ready, I will be here."
Support self-efficacy. Remind them that millions of people have quit successfully and that you believe they can do it when the time is right.
The board trap: a patient in precontemplation says they do not want to quit. The wrong answer is prescribing varenicline. The right answer is motivational interviewing. Match the intervention to the stage.
5 / 7
Relapse and Re-engagement
When the Patient Slips
The average smoker makes 8-11 attempts before maintaining long-term abstinence. Relapse is the expected course, not a sign of failure.
The boards test whether you abandon the patient or re-engage. The answer is always re-engage. Normalize the slip. Maintain pharmacotherapy. Arrange follow-up within the week. Shame is the biggest barrier to re-engagement.
A 47-year-old woman quit smoking 6 weeks ago after starting varenicline. She calls to report she smoked 3 cigarettes during a family argument last weekend. She feels ashamed and says "I guess I'm a hopeless case." What is the most appropriate next step?
Pregnancy: NRT is the only pharmacotherapy option. Varenicline and bupropion are not recommended. Behavioral counseling is first-line. NRT (short-acting forms preferred over patch) only if counseling alone is insufficient.
Psychiatric comorbidity: Smoking rates are 2-3x higher in patients with depression, anxiety, and schizophrenia. Varenicline and bupropion are both safe in stable psychiatric illness (EAGLES trial, 2016). Bupropion has the added benefit of treating underlying depression. Do not withhold pharmacotherapy from psychiatric patients.
Cardiovascular disease: NRT is safe in stable cardiovascular disease. The risk of continued smoking far exceeds any theoretical NRT risk. Varenicline is also safe and effective in this population.
A 34-year-old woman who is 14 weeks pregnant smokes half a pack per day. She has tried to quit with behavioral counseling alone for 4 weeks but continues to smoke. She asks about pharmacotherapy. What is the most appropriate agent?
Varenicline
Bupropion
Nicotine gum or lozenge
No pharmacotherapy; continue counseling only
6 / 7
Board Walkthrough
Board-Style Vignettes
Original clinical vignettes. One at a time. Tap to reveal the teaching chain after you answer.
VIGNETTE 1 OF 7
Right-click (or long-press) any option to cross it out. Double-click to highlight.
7 / 7
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last reviewed June 2026
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.