A, D, E, and K dissolve in fat and accumulate in tissue. Toxicity is a real clinical event, and deficiency takes weeks to develop because the body has reserves. Both are high-yield.
Vitamin Dossiers
The Fat Four
A, D, E, K: absorption depends on bile, stored in fat, and can reach toxic levels
⚡
A, D, E, K are fat-soluble. They need bile for absorption, store in adipose tissue, and unlike water-soluble vitamins can accumulate to toxic concentrations. Fat malabsorption states (cystic fibrosis, celiac, Crohn, biliary obstruction) deplete all four simultaneously.
👁
Vitamin A
Retinol · Retinal · Retinoic Acid
Key RolesNight vision (retinal + opsin = rhodopsin in rod photoreceptors) · Epithelial cell differentiation · Immune function · Mild antioxidant
ClinicalOral isotretinoin for cystic acne = concentrated Vitamin A · All-trans retinoic acid (ATRA) for APL (t15;17, PML-RAR fusion)
Night blindness is the earliest and most tested sign. Retinal is required to regenerate rhodopsin after light exposure. Without it, rod photoreceptors cannot re-sensitize in dim light.
Progression: Night blindness → Bitot spotsFoamy white patches of keratinized debris on the temporal conjunctiva. They are the first visible sign of xerophthalmia and indicate squamous metaplasia from Vitamin A deficiency. on conjunctiva (squamous metaplasia) → Corneal ulceration (keratomalacia) → Blindness.
Also: dry scaly skin, impaired wound healing, immune dysfunction. In children with measles, give Vitamin A: regenerates the destroyed respiratory epithelium and significantly reduces mortality.
Pseudotumor cerebri (idiopathic intracranial hypertension):
• Headache + papilledemaBilateral optic disc swelling from elevated intracranial pressure. Fundoscopy shows blurred disc margins. Main complication = blindness. Different from optic neuritis which is painful and typically unilateral.
• CT brain: normal (no mass, no hydrocephalus) = safe to proceed to LP
• LP: elevated opening pressure (>20 cm H2O) confirms diagnosis
Vitamin A excess also causes: hypercalcemia (direct osteoclast activation), bone pain, liver toxicity, and teratogenicity (why isotretinoin requires pregnancy testing).
Most common cause of pseudotumor cerebri: obesity. #2: Vitamin A excess.
☀️
Vitamin D
Cholecalciferol (D3) · Calcitriol (active)
Key RolesCa and PO4 absorption from gut (same direction: both up) · Bone mineralization · Phosphorus regulation
ActivationSkin (UV) → Liver (25-hydroxylation) → Kidney1-alpha hydroxylase in the kidney performs the final activation step. This enzyme is stimulated by PTH and low Ca/PO4. CKD destroys this step, causing secondary hyperparathyroidism. (1-alpha-hydroxylation) → Active calcitriol
Adults:Osteomalacia · soft bones, bone pain, proximal muscle weakness, fractures
Labs: Ca low, PO4 low (same direction = Vitamin D), PTH elevated (secondary), ALP elevated
At risk: CKD (no kidney 1-alpha-hydroxylase), dark skin + northern climate, malabsorption (Crohn, celiac), exclusively breastfed infants without supplementation
Sarcoidosis trap: granuloma macrophages carry autonomous 1-alpha-hydroxylase. They convert 25-OH-D to calcitriol without feedback inhibition, causing hypercalcemia with PTH suppressed and 25-OH-D normal but 1,25-(OH)2-D elevated.
Key distinction: In Vitamin D toxicity, Ca and PO4 are BOTH elevated (same direction). In primary hyperPTH, Ca is up but PO4 is down (opposite directions).
🛡
Vitamin E
Tocopherol · The Major Antioxidant
Key RoleTHE major antioxidant · protects cell membranes (especially RBCs) from free radicalReactive oxygen species that peroxidize membrane phospholipids. Vitamin E donates a hydrogen atom to neutralize them, protecting the cell membrane from oxidative chain reactions. damage · Works synergistically with selenium
clinical medicine NoteVitamin E = major antioxidant. Vitamin A = only mild antioxidant. This distinction is frequently tested.
Without membrane protection:
• Hemolytic anemia (RBC membranes burst, especially in premature newborns who have low fat stores)
• Posterior column + spinocerebellar tract degeneration → ataxia, loss of proprioception (looks neurologically identical to B12 deficiency)
At risk: Premature infants (most classic), fat malabsorption (CF, celiac, abetalipoproteinemia). Abetalipoproteinemia blocks chylomicron assembly; no fat-soluble vitamin transport = profound E deficiency.
The posterior column degeneration in Vitamin E deficiency is mechanistically similar to B12 deficiency (both impair myelin in the dorsal columns), but the lab test for B12 and MMA will be normal.
🩸
Vitamin K
Phylloquinone (K1) · Menaquinone (K2)
Key RoleGamma-carboxylationAdds a third carboxyl group to glutamic acid residues on clotting factors. Each factor has 10 glutamic acids, each getting carboxylated to generate 30 negative charges that attract calcium. Without calcium, the factors cannot localize to platelets and form a clot. of clotting factors 2, 7, 9, 10 + Protein C and Protein S (remember: 1972)
SourceGut flora produces 90% of K2 · Leafy greens provide K1 · Newborns born with sterile gut = zero flora
PT/INR elevated (Factor 7 has shortest half-life at 4-6 hours, disappears first)
Bleeding: easy bruising, mucosal bleeding, hemorrhage
At risk:
• Newborns: sterile gut, no flora to make K2. Every newborn gets IM Vitamin K at birth to prevent hemorrhagic disease of the newborn (day 2-3)
• Prolonged antibiotics: kill gut flora
• Fat malabsorption
• Warfarin use (blocks K epoxide reductase)
Reversal: Vitamin K IM or PO (takes 6-24 hrs) vs FFP (immediate, for active life-threatening bleeding)
Warfarin skin necrosis: Protein C (also vitamin K-dependent, half-life 6 hrs) disappears before the clotting factors do. Starting warfarin without heparin bridge creates a transient hypercoagulable window that can cause microvascular thrombosis and skin necrosis.
From the Attending
The fat-soluble vitamins are four separate clinical entities that board writers love to blur together. The testable patterns: Vitamin A deficiency = night blindness first, toxicity = pseudotumor cerebri. Vitamin D deficiency = Ca and PO4 both low (same direction), CKD breaks the activation step. Vitamin E = the antioxidant, deficiency = hemolytic anemia in premature infants plus ataxia. Vitamin K = coagulation, warfarin blocks it, newborns need it at birth. Know which one first.
Interactive
Vitamin D Activation Pathway
Tap each node to reveal what happens at each step
⚠️
CKD destroys the kidney step. No 1-alpha-hydroxylase means no active calcitriol → Ca absorption falls → secondary hyperPTH → phosphate retention. Result: Ca low, PO4 high, PTH high. Treat with calcitriol (the active form) directly, bypassing the broken kidney step.
Clinical Images
What You See at the Bedside
Tap to enlarge. Recognize the clinical phenotype of fat-soluble vitamin deficiency states.
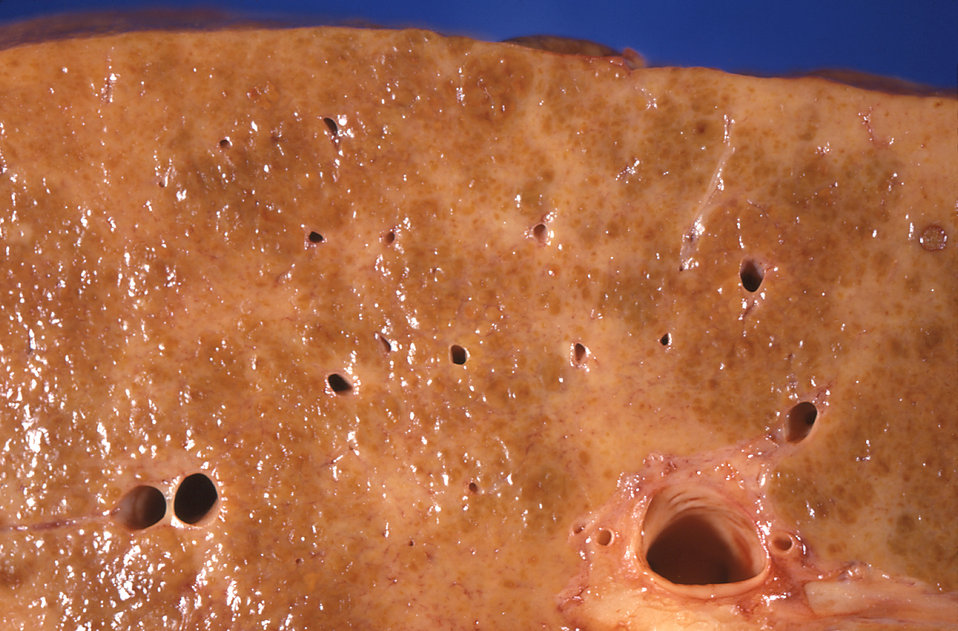
Scleral icterus · liver disease impairs all fat-soluble vitamins
Alcoholic cirrhosis · depletes A, D, E, K simultaneously
High-Yield Rule
Ca and PO4 Direction
Same direction = Vitamin D. Opposite directions = PTH or PTH resistance.
Condition
Ca
PO4
PTH
Pattern
Vitamin D excess
↑
↑
↓
Same direction
Vitamin D deficiency
↓
↓
↑
Same direction
Primary hyperPTH
↑
↓
↑
Opposite
Vitamin A excess (osteoclast activation)
↑
↓
↓ (suppressed)
Opposite
CKD (no 1-alpha-hydroxylase)
↓
↑
↑
Opposite + high PO4
Sarcoidosis (ectopic calcitriol)
↑
↑
↓
Same (PTH suppressed)
💡
The rule that never fails: If Ca and PO4 move in the same direction, the problem is Vitamin D (or an entity that mimics it, like sarcoidosis). If they move in opposite directions, PTH or PTH resistance is driving it.
Deep Dive
Vitamin K and the Warfarin Problem
Why bridging with heparin exists, and what happens when you skip it
From the Attending
Vitamin K gamma-carboxylates factors 2, 7, 9, 10 and Protein C/S. Warfarin blocks vitamin K recycling. Protein C has the shortest half-life (6 hours) of all the vitamin K-dependent proteins. Start warfarin without heparin, and Protein C vanishes before the clotting factors do: a transient hypercoagulable window opens. This is why every board question about skin necrosis 6-24 hours after starting warfarin points to Protein C deficiency. Know your half-lives.
Hour 0: Start warfarin
All factors at 100%. The clock starts ticking on half-lives.
Tap to expand
Warfarin blocks vitamin K epoxide reductase, preventing regeneration of active vitamin K. The liver can no longer gamma-carboxylate new clotting factors. But the factors already in the blood are still functional. Now it is a race of half-lives.
Hour 6: DANGER ZONE
Protein C (half-life 6 hrs) is 50% gone. Clotting factors? Still mostly fine.
Tap to expand
Protein C is an anticoagulant. Its half-life is 6 hours, shorter than Factor VII (4-6 hours clotting factor, but Protein C degrades even faster in some individuals). When Protein C disappears before the pro-coagulant factors, the net balance tips toward clotting: a transient hypercoagulable state. If the patient has underlying Protein C deficiency, this tipping happens faster and more severely, causing microvascular thrombosis and skin necrosis.
Hour 6+: Heparin bridges the gap
Heparin activates antithrombin III immediately, covering the window.
Tap to expand
Heparin (half-life 1-2 hours for UFH) activates antithrombin III, which blocks thrombin and factors IX, X, XI, and XII. This provides immediate anticoagulation while Protein C is depleted and before warfarin has eliminated enough clotting factors. UFH is monitored by PTT; LMWH does not require monitoring.
Day 2-5: Warfarin reaches steady state
INR therapeutic. Heparin is discontinued only when INR is stable at target.
Tap to expand
Factor VII (shortest clotting factor half-life at 4-6 hours) disappears first, causing PT to rise. But full anticoagulation requires Factors II, IX, and X to also be depleted. This takes 2-5 days of warfarin. The INR target for most indications is 2-3. Keep heparin until INR has been therapeutic for at least 24-48 hours on two consecutive measurements.
💡
Warfarin vs Heparin at a glance: Warfarin = oral, blocks vitamin K recycling, monitored by PT/INR, crosses placenta (teratogenic). Heparin = IV or SubQ, activates antithrombin III, monitored by PTT, does NOT cross the placenta (safe in pregnancy). Reversal: warfarin = Vitamin K IM + FFP if bleeding; heparin = protamine sulfate.
Symptom Detective
Which Vitamin Is Deficient?
Follow the symptoms to the diagnosis. Tap an option to navigate.
The patient has a fat-soluble vitamin deficiency. Which finding is most prominent?
Night blindness + dry eyes suggests a deficiency in which vitamin?
Correct: Vitamin A. Retinal (the aldehyde form of Vitamin A) combines with the protein opsin to form rhodopsin in rod photoreceptors. Without it, rods cannot re-sensitize in dim light. Night blindness is the earliest sign. Bitot spots (foamy conjunctival plaques from squamous metaplasia) follow. End-stage: corneal ulceration and blindness.
The rule: night blindness = Vitamin A first, always.
Not quite. Vitamin D deficiency causes bone problems (rickets, osteomalacia) and calcium dysregulation, not visual symptoms. Night blindness is specific to Vitamin A deficiency because retinal is the chromophore in rhodopsin.
Not quite. Vitamin E deficiency causes hemolytic anemia and spinocerebellar degeneration (ataxia, loss of proprioception), not night blindness or eye dryness.
Bone softening with low Ca and low PO4 (both moving together). Which vitamin?
Correct: Vitamin D. Ca and PO4 moving in the same direction (both low in deficiency, both high in toxicity) is the Vitamin D pattern. In children: rickets (bowed legs, rachitic rosary, craniotabes). In adults: osteomalacia (bone pain, proximal muscle weakness, pseudofractures on X-ray). Secondary hyperPTH drives the PTH up.
The rule: Ca and PO4 same direction = Vitamin D.
Not this one. Vitamin A excess causes bone pain via osteoclast activation, but Ca goes up and PO4 goes down (opposite directions) because PTH is suppressed. Vitamin A deficiency does not primarily cause bone softening.
Not this one. Vitamin K deficiency causes clotting factor deficiency and bleeding. It does not cause bone softening or abnormal Ca/PO4 levels.
PT elevated, normal platelet count. Which vitamin is deficient?
Correct: Vitamin K. Vitamin K enables gamma-carboxylation of factors 2, 7, 9, and 10. Factor 7 has the shortest half-life (4-6 hours) among clotting factors, so PT/INR rises first. Platelets and fibrinogen are normal (platelet plug is intact). Classic scenarios: newborn on day 2 of life (no gut flora yet), patient on prolonged antibiotics, fat malabsorption.
The rule: elevated PT with normal platelet count and fibrinogen = Vitamin K deficiency until proven otherwise.
Not quite. Vitamin E deficiency causes hemolytic anemia (membrane fragility) and neurological degeneration, not coagulopathy. PT and PTT would be normal in Vitamin E deficiency.
Not this one. Vitamin D deficiency causes rickets and hypocalcemia, not clotting factor deficiency. An elevated PT with normal platelet count should direct you to Vitamin K or the liver (which synthesizes the clotting factors).
Ataxia + loss of proprioception + hemolytic anemia in a premature infant. Which vitamin?
Correct: Vitamin E. Tocopherol is the major antioxidant protecting cell membranes from lipid peroxidation. Premature infants are born with minimal adipose stores and therefore minimal Vitamin E reserves. Without membrane protection: RBCs lyse (hemolytic anemia, negative Coombs) and posterior column + spinocerebellar tracts demyelinate (ataxia, proprioception loss). This is clinically indistinguishable from B12 neurological deficiency.
The rule: hemolytic anemia + ataxia + proprioception loss in a premature infant = Vitamin E deficiency.
Not this one. Vitamin A deficiency causes night blindness, xerophthalmia, and immune impairment. Neurological degeneration and hemolytic anemia are not the primary features of Vitamin A deficiency.
Not quite. Vitamin K deficiency causes coagulopathy (elevated PT/INR, bleeding) because clotting factors cannot be gamma-carboxylated. It does not cause ataxia or hemolytic anemia.
Sort Challenge
Fat-Soluble or Water-Soluble?
Drag each vitamin to the correct column. On mobile, tap to select then tap a column.
Vitamin A
Vitamin C
Vitamin D
Folate (B9)
Vitamin E
Thiamine (B1)
Vitamin K
Niacin (B3)
B12
🌎 Fat-Soluble
💧 Water-Soluble
Board Walkthrough
Vignette Drill
6 original clinical vignettes, shuffled each session. Cross out distractors before committing.
Question 1 of 6
correct out of 6
Medically reviewed by Fatima Ali, DO and Kaitlyn Cocuzzo, MD · Last updated July 6, 2026 at 12:11 AM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.