Zinc heals wounds, copper builds connective tissue, selenium guards the heart. Each deficiency has a signature clinical picture the clinical medicine love to disguise as something else.
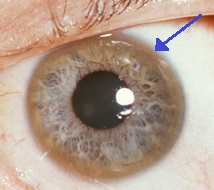
Copper deposits in Descemet membrane of the cornea. Visible as golden-brown rings on slit-lamp exam. Pathognomonic for copper overload.
Tap any image to enlarge. Photos via Wikimedia Commons.
Section I
🪛 The Minerals
Tap any element to expand its full clinical profile.
20
Ca
Calcium
12
Mg
Magnesium
30
Zn
Zinc
29
Cu
Copper
26
Fe
Iron
What It Does
Intracellular calcium triggers all muscle contraction
Only two membranes depolarize using calcium instead of sodium: atrium and thalamus🔑A-T for Atrium-Thalamus: the two rebels that depolarize with Ca2+ instead of Na+.
Cardiac ventricle uses calcium-induced calcium releaseSmall amount of extracellular Ca2+ enters through L-type channels during the plateau phase, then triggers massive Ca2+ release from the sarcoplasmic reticulum via ryanodine receptors.
Presynaptic influx required for release of all neurotransmitters
Required for normal bone and teeth development
Clinical Pearl
Babies in utero need calcium for neurotransmitter release -> deficiency can cause developmental delay
What It Does
Cofactor for ALL kinases(why?)Kinases need ATP. Mg2+ stabilizes the negative charges on ATP's phosphate tail so the kinase can work. No Mg = no kinase activity.
Cofactor for PTH -> low Mg can mimic hypoparathyroidism
Cotransporter with K+ in the early distal convoluted tubule
Board Trap
Can't fix hypokalemia until you fix hypomagnesemia -> they share a cotransporter in the DCT. If Mg is low, K+ keeps leaking out no matter how much you replace.
What It Does
Needed by hair, skin, sperm, taste buds, and 100+ enzymes
🔑Zinc = the vanity mineral. Hair, skin, taste, and swimmers. Everything you'd notice on a date.
Forms zinc finger domains in transcription factors -> zinc plays a role in DNA binding
Cofactor for collagenase (remodeling phase of wound healing)
Deficiency
Dysgeusia (altered taste) and anosmia
Alopecia, delayed wound healing, male hypogonadism
Ferrous iron (Fe2+) binds oxygen -> the functional form
Ferric iron (Fe3+) is oxidized -> cannot bind oxygen
🔑Fe2+ = ferrOUS = useOUS. Fe3+ = ferrIC = useless IC.
Vitamin C keeps iron in Fe2+ state for GI absorption
Hepcidin
Hepcidin is a liver peptide that blocks ferroportin (iron exporter on enterocytes and macrophages)
Iron high -> hepcidin rises -> ferroportin blocked -> iron trapped in enterocytes (shed in stool) and macrophages -> less circulating iron
Anemia of chronic disease: inflammation -> IL-6 -> hepcidin -> iron sequestered in macrophages -> low serum iron BUT high ferritin
Board trap: low serum iron + HIGH ferritin = anemia of chronic disease; low serum iron + low ferritin = true iron deficiency
Section II
🔬 Trace Elements
Tiny amounts, massive consequences. Each has a single board association.
24
Cr
Chromium
34
Se
Selenium
42
Mo
Molybdenum
25
Mn
Manganese
9
F
Fluoride
What It Does
Enhances insulin action -> delays progression of diabetes
Deficiency
Impaired glucose tolerance / diabetes -> seen in clinical practice in long-term TPN without trace minerals
🔑Chromium = Chrome = shiny insulin receptors. No chrome, receptors go dull. Glucose spikes.
What It Does
Essential cofactor for glutathione peroxidase -> antioxidant defense
Needed primarily by the heart
Deficiency: Keshan Disease
Dilated cardiomyopathy -> endemic in selenium-poor soils of rural China; also seen in long-term TPN
Excess
Garlic-smelling breath (arsenic also does this)
🔑Se-lenium and Arsenic: the two garlic-breath cousins. Se-licious.
What It Does (with Manganese)
Needed by enzymes in glycolysis
Both xanthine oxidase needs molybdenum AND manganese
(why it matters)Xanthine oxidase converts hypoxanthine to xanthine to uric acid. Allopurinol blocks this enzyme to treat gout.
What It Does
Needed by enzymes in glycolysis
Partners with molybdenum for xanthine oxidase (uric acid production)
What It Does
Needed for teeth and bone development and hardening
Excess / Poisoning
Blocks enolase of glycolysis -> ATP famine
(connection!)Enolase converts 2-phosphoglycerate to PEP in glycolysis. Block it and you choke off ATP production. Rapidly dividing cells die first.
X-ray: bright, shiny teeth and bones; horizontal white and dark lines in teeth (dental fluorosis)
Death from heart failure (heart needs constant energy)
From the Attending
The clinical medicine love to disguise Wilson disease. You will see a young patient with either liver disease or psychiatric symptoms or a movement disorder, and you have to connect all three. The trick: any young patient with a movement disorder that looks like Parkinson gets a slit-lamp exam and a ceruloplasmin level before anything else. That's the diagnosis you cannot miss. Hemochromatosis similarly hides in plain sight: bronze skin + diabetes + joint pain in a middle-aged man is the bronze diabetes triad. The HFE mutation, serial phlebotomy as treatment, and the distinction from secondary hemochromatosis (treat with chelation, not phlebotomy) are all high-yield. Know your clues. Every time.
Copper Transport
Copper Metabolism: Normal vs Wilson Disease
Watch copper move through the body. Toggle between normal transport and Wilson disease to see where the pathway breaks.
Copper Pathway: Live Animation
Animated: copper absorption, ceruloplasmin binding, and deposition pattern in disease.
Board Favorite
Wilson Disease vs Huntington Disease
Both cause movement disorders with psychiatric symptoms in a younger patient. The liver and eyes tell you which is which.
Feature
Huntington Disease
Wilson Disease
Inheritance
Autosomal dominant
Autosomal recessive
Genetic cause
CAG trinucleotide repeats -> caudate atrophy
ATP7B mutation -> copper accumulation
Age of onset
30-50s (anticipation)
Before 40 (often 5-35)
Movement
Chorea
Tremor, dysarthria, dystonia
Liver disease?
No
Yes: cirrhosis, liver failure
Eye finding?
None
Kayser-Fleischer rings
Lab finding
None specific
Low ceruloplasmin, high urine copper
Treatment
Dopamine blockers (symptom management)
Penicillamine, trientine, zinc
Most common cause of death
Suicide, aspiration pneumonia
Liver failure
Huntington Disease
InheritanceAutosomal dominant
Genetic causeCAG repeats → caudate atrophy
Age of onset30-50s (anticipation)
MovementChorea
Liver diseaseNo
Eye findingNone
LabNone specific (tap)
TreatmentDopamine blockers (tap)
DeathSuicide, aspiration pneumonia (tap)
Wilson Disease
InheritanceAutosomal recessive
Genetic causeATP7B mutation → copper buildup
Age of onsetBefore 40 (often 5-35)
MovementTremor, dysarthria, dystonia
Liver diseaseYes: cirrhosis, liver failure
Eye findingKayser-Fleischer rings
LabLow ceruloplasmin, high urine copper (tap)
TreatmentPenicillamine, trientine, zinc (tap)
DeathLiver failure (tap)
💡 ATP7A vs ATP7B
ATP7A defect = Menkes disease = copper Absent from body (X-linked recessive, infant onset).
ATP7B defect = Wilson disease = copper Builds up in tissues (autosomal recessive, young adult onset).
Challenge
Which Deficiency?
Work through the clinical clues one step at a time before seeing the answer.
🎯 Clinical Identification Challenge
An infant is brought in for brittle, depigmented, coarse hair and new seizures. Serum copper is 36 mcg/dL (70-140 mcg/dL). Which deficiency is causing this presentation?
A patient on long-term TPN for 10 weeks develops new-onset glucose of 298 mg/dL with no prior history of diabetes. TPN was formulated without trace elements. Which deficiency explains this?
A 28-year-old woman presents with dysarthria, resting tremor, and elevated liver enzymes. She has no family history of movement disorders. Serum ceruloplasmin is 10 mg/dL (normal 20-40 mg/dL). What is the most likely diagnosis and which diagnostic test confirms it?
Test Yourself
🎮 Match the Mineral
Drag each mineral to its signature finding. Tap to select and tap the target on mobile.
Mineral
Signature Finding
Board Walkthrough
🎯 3rd-Order Vignettes
Six original clinical vignettes. One at a time. Answer, then read the explanation. The teaching chain drops after each one.
VIGNETTE 1 OF 6
All 6 vignettes complete. Shuffle and run them again any time.
Medically reviewed by Fatima Ali, DO and Kaitlyn Cocuzzo, MD · Last updated July 6, 2026 at 12:11 AM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.