The leg that hurts more the longer you stand on it.
Broken valves, pooling blood, and skin that tells the whole story
before you ever order a test.
↓ scroll to learn
Clinical Challenge
A 54-year-old woman presents with a
dull, heavy aching in her left leg
for the past 6 months. The pain is worse at the end of the day
after prolonged standing, and improves with walking and leg elevation.
She has a history of deep vein thrombosis 2 years ago, treated
with a course of anticoagulants. Examination reveals
2+ pitting edema of the lower extremity,
reddish-brown discoloration above
the medial malleolus, scattered telangiectasias,
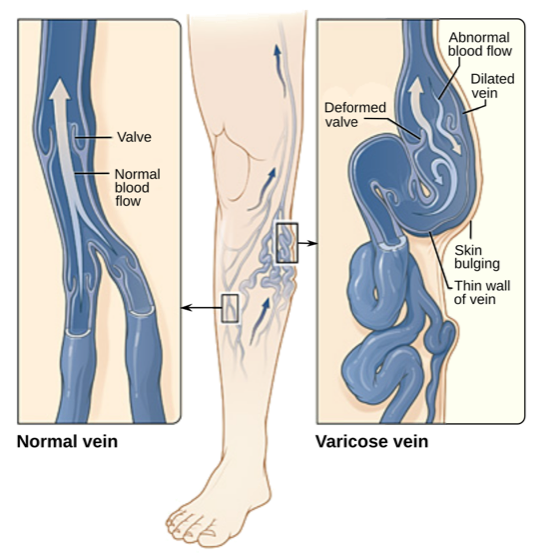
and prominent varicose veins.
What is the most appropriate next diagnostic step?
1
CVI vs PAD
Tap each row to reveal. clinical medicine love this comparison.
Venous
Chronic Venous Insufficiency
Pain Pattern tap
Dull, heavy aching. Worse at the end of the day after prolonged standing or sitting. Venous blood pools under gravity.
What helps tap
Elevation and walking (calf muscle pump squeezes blood back up). Think: gravity is the enemy, so fight gravity.
Skin findings tap
Hemosiderin staining (reddish-brown, medial ankle), varicose veins, telangiectasias, lipodermatosclerosis, venous ulcers at the medial malleolus.
Ulcer location tap
Medial malleolus. Shallow, irregular borders, moist base. Often painless or mildly painful. (Venous = Medial; think "V for Ventral/Medial.")
Pulses tap
Normal. The arterial system is fine. The problem is veins failing to return blood.
First-line test tap
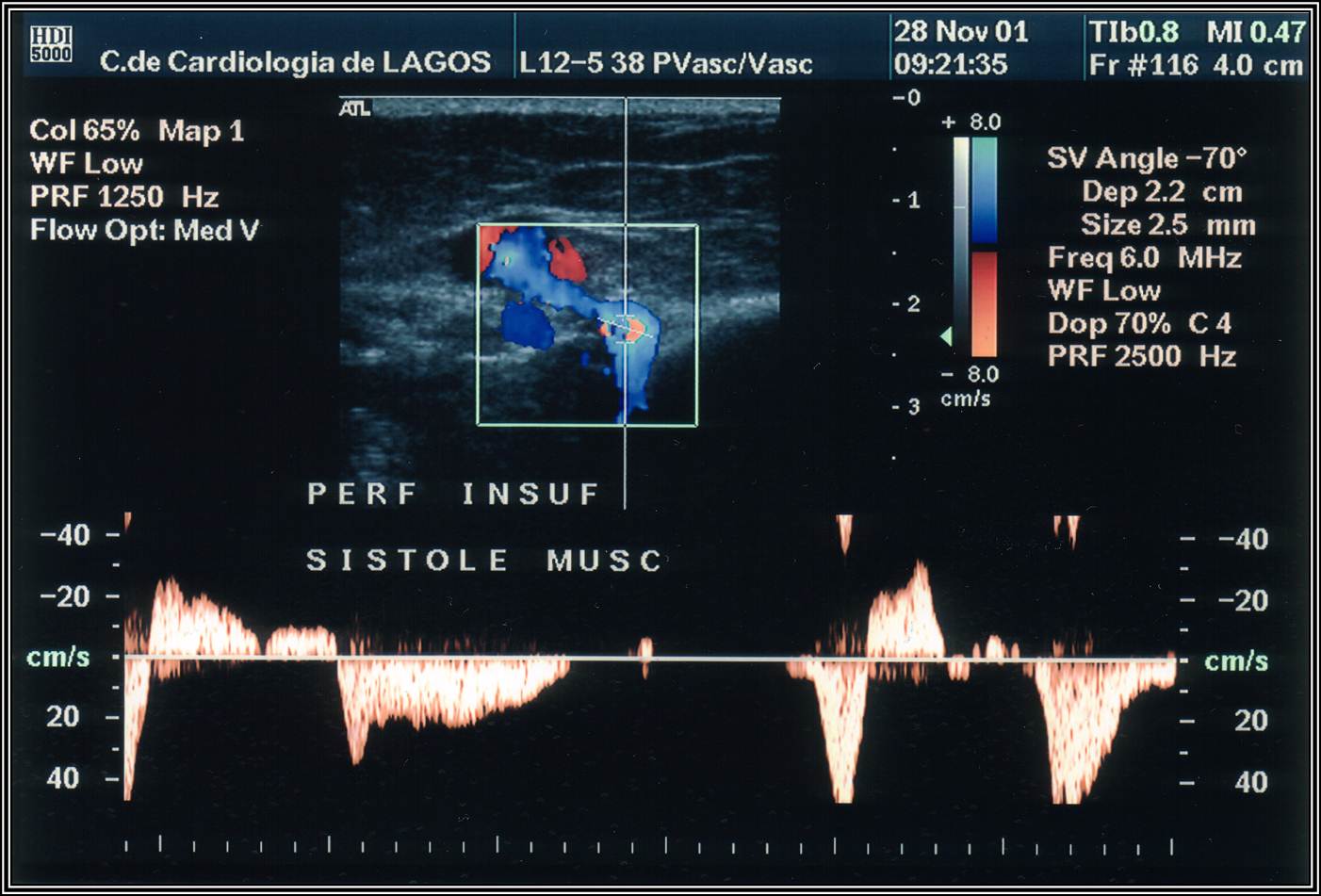
Duplex ultrasonography. Shows valve incompetence and reflux duration. Gold standard.
Arterial
Peripheral Arterial Disease
Pain Pattern tap
Intermittent claudication. Sharp, cramping pain in calves/thighs during walking. Muscles starved of oxygen mid-exercise.
What helps tap
Rest (stopping walking). Elevation makes it WORSE (decreases arterial perfusion). Think: demand exceeds supply, so stop the demand.
Skin findings tap
Thin, shiny, hairless skin. Pale or cyanotic on elevation. Dependent rubor. Cool extremity. Nail dystrophy. No hemosiderin staining.
Diminished or absent. Dorsalis pedis and posterior tibial pulses weak or gone. This is the giveaway.
First-line test tap
Ankle-brachial pressure index (ABPI). Normal 0.9-1.3. Below 0.9 = PAD. Below 0.4 = critical limb ischemia.
The clinical practice Split:
CVI pain is worse at end of day, relieved by elevation.🔑Elevation helps Venous = Every Valve. Gravity drains the broken valves when you lift the leg.
PAD pain is worse with walking, relieved by rest.🔑Rest relieves Arterial = Restop All demand. Stop walking, stop needing O2, stop the pain.
If the stem says "elevation helps," it is venous. If the stem says "rest helps," it is arterial.
Trap: Post-thrombotic syndrome.🔑Post-Thrombotic = Permanently Trashed valves. The clot left, the damage stayed. Duplex US, not D-dimer.
A patient with prior DVT who now has chronic leg swelling and skin changes = CVI from valve damage, NOT a new DVT. Do not order D-dimer. Order duplex US.
2
Workup Decision Tree
A patient walks in with leg pain. Work through the diagnostic pathway.
👥
A 58-year-old man complains of bilateral leg pain that has worsened over months.
His legs feel "heavy and swollen" by evening.
He works as a grocery store cashier (stands all day).
What is the most likely pattern?
Venous insufficiency pattern: worse with standing, better with elevation
Arterial claudication pattern: worse with walking, better with rest
Neuropathic pattern: burning/tingling regardless of position
🔍
You examine his legs. You find bilateral pitting edema,
brownish pigmentation near both ankles,
and a few tortuous superficial veins.
Pedal pulses are 2+ bilaterally.
Which finding MOST supports CVI over PAD?
Bilateral pitting edema
Normal pedal pulses with hemosiderin staining
Tortuous superficial veins
🔬
You suspect CVI. Time to confirm.
What do you order first?
CT venography
D-dimer
Duplex ultrasonography with Valsalva
Ankle-brachial pressure index
📈
The duplex US report reads: "Reflux duration >0.5 seconds in the great saphenous vein
with Valsalva maneuver. Incompetent valves at the saphenofemoral junction."
This confirms:
Acute deep vein thrombosis
Chronic venous insufficiency with saphenous reflux
Superficial thrombophlebitis
💊
CVI confirmed. The patient asks what he can do.
His CEAP class is C3 (edema without skin changes beyond pigmentation).
What is the first-line treatment?
Surgical vein stripping
Endovenous laser ablation
Graduated compression stockings + leg elevation + exercise
Anticoagulation with warfarin
CEAP Classification
CEAP (Clinical, Etiologic, Anatomic, Pathophysiologic) grades CVI severity.
Tap each class to see the details.
C0No visible or palpable venous disease
Normal exam. Patient may still have symptoms (heaviness, aching) but nothing you can see or feel. Duplex US can still show reflux at this stage.
C1Telangiectasias or reticular veins
Spider veins (telangiectasias less than 1mm) and reticular veins (1-3mm). Cosmetic concern mostly. Not dangerous on their own but signal underlying reflux.
C2Varicose veins (3mm or larger)
Dilated, tortuous subcutaneous veins. The classic "ropey" veins you can see bulging under the skin. Usually the great saphenous vein territory.
C3Edema
Pitting edema from venous hypertension forcing fluid into interstitial space. Worse at end of day. Improves overnight with elevation. This is where compression stockings become essential.
Previous ulcer that has closed. Still has skin changes. High risk of recurrence without ongoing compression therapy and surveillance.
C6Active venous ulcer
Open ulcer, typically at the medial malleolus. Shallow, irregular borders, moist base. Managed with compression bandaging, wound care, and treating the underlying reflux. Most severe clinical stage.
Tap each card to flip. Each one is a distinct complication with its own board signature.
🦵
Venous Stasis Ulcer
C6 · Medial Malleolus
tap to flip →
Board Signature
Shallow, moist, irregularly-bordered ulcer at the medial malleolus. Painless or mildly painful. Granulating base.
Mechanism: venous hypertension forces fluid and RBCs out of capillaries. Tissue breaks down when it can no longer heal faster than it leaks.
CEAP C6 · preserved pulses · duplex US to confirm reflux
🪖
Lipodermatosclerosis
C4b · Fibrosis
tap to flip →
Board Signature
Skin hardens and contracts above the medial ankle, creating the classic "inverted champagne bottle" shape. The leg is narrow at the ankle, wide above.
Mechanism: chronic inflammation from hemosiderin triggers fibroblast activation and subcutaneous fibrosis. Skin literally tightens.
C4b · pre-ulcer warning · not cellulitis (no warmth, no fever)
🧵
Varicose Veins
C2 · Saphenous Territory
tap to flip →
Board Signature
Dilated, tortuous subcutaneous veins ≥3mm. Usually in the great saphenous vein territory. Visible bulging under skin.
Mechanism: valve incompetence lets blood reflux backward. Pressure builds, vein walls weaken, and the vessel dilates and torques under the skin.
C2 · aching, heaviness · thrombophlebitis risk · duplex US for reflux
🩸
Post-Thrombotic Syndrome
DVT → CVI
tap to flip →
Board Signature
DVT scars and destroys venous valves. Weeks to months later: unilateral chronic edema, hemosiderin staining, and eventually ulceration in the same leg as the original clot.
The board trap: a patient with prior DVT who develops chronic leg changes is NOT having another DVT. Do NOT order D-dimer. Order duplex US.
Non-pitting + toes involved + no hemosiderin = lymphedema, not CVI
Clinical Images
📷 Venous ulcer · medial malleolus
📷 Varicose veins · tortuous, C2
📷 Lipodermatosclerosis · C4b fibrosis
📷 Duplex US · gold-standard test
Pattern lock:
Varicose veins (C2) → edema (C3) → hemosiderin + lipodermatosclerosis (C4) → healed ulcer (C5) → active ulcer (C6).
The CEAP class always describes the worst current finding.
4
Management Pathway
Bilateral leg swelling just walked in. Work through the staging and treatment decision.
🥥
A 62-year-old man has bilateral leg swelling for 4 months. It worsens at the end of the day and improves overnight. No shortness of breath, no JVD, no orthopnea. Pedal pulses intact.
What is the most likely etiology of his bilateral leg swelling?
You suspect CVI. On exam: bilateral pitting edema to mid-calf, hemosiderin staining at both medial ankles, tortuous veins on both legs, normal heart sounds, no JVD. No signs of systemic disease.
What confirms venous insufficiency and defines the anatomic level of reflux?
Duplex ultrasonography: identifies reflux duration and site of valve incompetence
BNP level: rules out heart failure as the cause
Venography: maps the venous system with contrast
📊
Duplex confirms bilateral great saphenous reflux. He has pitting edema (C3), hemosiderin staining (C4a), and one healed ulcer site on the right (C5). No active ulcer.
What CEAP class should you assign?
C3: assign the most common finding present
C5: assign the highest (worst) CEAP class present
C4a: the healed ulcer is no longer an active problem
💊
CEAP C5. He is symptomatic and motivated. You have already confirmed saphenous reflux on duplex.
After 3 months of compression therapy with continued symptoms, what is the next step?
Increase compression to 40-50 mmHg and re-evaluate in 6 months
Start anticoagulation with warfarin for venous reflux
Endovenous ablation (EVLA or RFA) of the incompetent saphenous vein
5
Quiz
5 random questions from a pool of 10. All original.
Try Again
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 2, 2026 at 4:50 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.