Every board question about valvular disease ends the same way: "Which hemodynamic parameter is changed?" This page turns those parameters into something you can see, sort, and eliminate until the right answer is the only one left.
scroll to play
0
Challenge Before Reveal
A stiff outlet valve makes the ventricle generate more pressure before blood leaves. Choose the parameter before revealing the chain.
Fixed outflow obstruction means the LV pushes against a tighter exit. That is afterload.
A leaky valve sends blood back into the ventricle during diastole. Choose the remodeling pattern before revealing the chain.
Chronic extra volume stretches the chamber. Sarcomeres add in series, so the ventricle dilates.
💡Read every stem the same way: first decide whether the problem is inflow, outflow, squeeze, leak, or vascular tone. Then the parameter becomes predictable.
1
The Master Equation
Everything in hemodynamics comes from one formula. Build it.
Build the Equation
CO=
?
×
?
HR
SV
MAP
SVR
💡CO = HR × SV. Cardiac output is the volume of blood pumped per minute. Normal: 4 to 8 L/min. Every hemodynamic question traces back to this.
Now the SV part. Three things control how much blood the ventricle ejects per beat:
Preload
tap to reveal
Preload = EDV
The stretch on the ventricle at end-diastole. More blood returns, more stretch, more force (Frank-Starling). Think of it as how far you pull back a rubber band before releasing.
Afterload
tap to reveal
Afterload = Wall Stress
The resistance the ventricle pushes against during ejection. For the LV, afterload is essentially SVR (systemic vascular resistance). For the RV, it is PVR (pulmonary vascular resistance). Higher afterload = harder to eject = lower SV.
Contractility
tap to reveal
Contractility = Intrinsic Force
The force the myocardium generates independent of stretch. Sympathetics and digoxin increase it. Beta-blockers and heart failure decrease it. On a PV loop, increased contractility shifts the end-systolic pressure-volume relationship (ESPVR) to the left.
Board Trap
They love to phrase it as "Which parameter is DECREASED in this patient?" and list preload, afterload, contractility, compliance, and SVR. If you can not define each one in one sentence, you are guessing.
2
Frank-Starling Law
More stretch = more force = more SV. But only up to a point.
Frank-Starling Curve · Wikimedia Commons
The normal heart sits on the steep part of the curve. Increased preload (more venous return) leads to a proportional increase in stroke volume. The failing heart operates on the flat portion: adding more volume does not increase output; it just causes congestion.
Elimination Round: Frank-Starling
Which of these shifts the Frank-Starling curve UPWARD (increased contractility at the same preload)? Eliminate the wrong ones.
💡Upward shift = more contractility (sympathetics, digoxin, dobutamine). Downward shift = less contractility (heart failure, beta-blockers, Ca2+ channel blockers). The curve POSITION changes, not the curve shape.
3
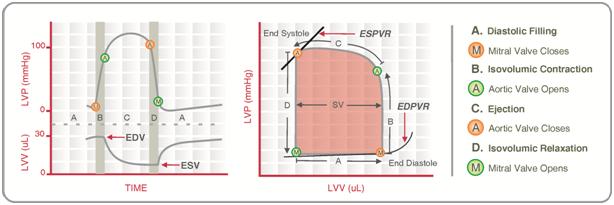
Pressure-Volume Loops
The PV loop is a map of one heartbeat. Once you can read it, every valvular question becomes visual.
Cardiac PV Loop · Wikimedia Commons
Interactive PV Loop Viewer
4
Valvular Lesion Parameters
This is what clinical medicine actually test. Not "what murmur is this," but "which parameter changes and how." Tap each card to see the hemodynamic profile.
Mitral StenosisLA pressure: Increased (blood can not cross valve) LV preload: Decreased (less filling) CO: Fixed (does not increase with exercise) Pulmonary pressure: Increased (backs up)
PV loop: smaller (less volume in, less volume out)
Sound: opening snap, diastolic rumble
Mitral Regurgitation
tap for parameters
Mitral RegurgitationLA pressure: Increased (v-wave on PCWP) LV preload: Increased (regurgitant volume returns next beat) Effective CO: Decreased
Hypertrophy: Eccentric (volume overload of LA + LV)
PV loop: total SV looks high, but forward flow is low
The v-wave is the signature finding
Parameter Match: Which Direction?
For each valvular lesion, assign the correct arrow to each parameter. Tap an arrow, then tap the slot to place it.
5
Concentric vs Eccentric
Pressure overload and volume overload remodel the heart differently. This is what clinical medicine mean by "which type of hypertrophy."
Concentric
Pressure overload
Sarcomeres added in parallel
Wall gets thicker, lumen stays same or shrinks
Seen in: aortic stenosis, chronic HTN
Compliance decreases (stiff wall)
Eccentric
Volume overload
Sarcomeres added in series
Chamber dilates, wall may thin
Seen in: aortic regurg, mitral regurg
Compliance increases (stretchy wall)
Elimination Round: Hypertrophy Type
Which conditions cause CONCENTRIC hypertrophy? Eliminate the ones that cause eccentric.
6
Compliance vs Elastance
These two terms are inverses. clinical medicine use them interchangeably to confuse you.
Compliance
tap to reveal
Compliance = ΔV / ΔP
How much volume change for a given pressure change. A compliant ventricle fills easily without a big pressure rise. Decreased compliance = diastolic dysfunction (HFpEF). The ventricle is stiff, so filling pressure rises for the same volume.
Elastance
tap to reveal
Elastance = ΔP / ΔV
The inverse of compliance. How much pressure rises for a given volume. High elastance = stiff ventricle = diastolic dysfunction. On a PV loop, the ESPVR slope IS elastance. Steeper slope = higher contractility = higher elastance.
Board Trap
"Which parameter is DECREASED?" If a patient has concentric hypertrophy with diastolic dysfunction, compliance is decreased and elastance is increased. They will put both in the answer choices. Read carefully: decreased compliance and increased elastance describe the same thing.
7
Shock: The Parameter Profiles
Every shock type has a hemodynamic fingerprint. Sort the scenarios into the right category.
Shock Sorter
Drag each scenario into the correct shock type. On mobile, tap a scenario then tap the category.
Cardiogenic
Distributive
Hypovolemic
Obstructive
💡The two big hemodynamic fingerprints to remember: Low CO + High SVR = cardiogenic or hypovolemic (body compensating). High CO + Low SVR = distributive (vessels are dilated, heart is pumping hard to compensate). Obstructive looks like cardiogenic but has a mechanical cause (PE, tamponade, tension pneumo).
8
SVR vs PVR
clinical medicine love to ask what increases or decreases each. Eliminate the wrong ones.
Elimination: What INCREASES SVR?
Eliminate everything that does NOT increase systemic vascular resistance.
Elimination: What INCREASES PVR?
Eliminate everything that does NOT increase pulmonary vascular resistance.
W
clinical Walkthrough
Five clinical vignettes. Each one ends with "which hemodynamic parameter is changed?" Read the stem, pick the answer, then see why the clues pointed there.
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.