Allergy and Immunology · Emergency
One antibody loads the gun, a second exposure pulls the trigger, and within minutes every system is failing at once. Learn the mast-cell chain, the two-system threshold, why epinephrine goes in the thigh first, and the bradykinin imposter that epinephrine cannot touch.
The Setup
Anaphylaxis is a single cell type, the mast cell, emptying its chemical warehouse all at once. Walk the chain from antibody to shock and the whole emergency lines up.
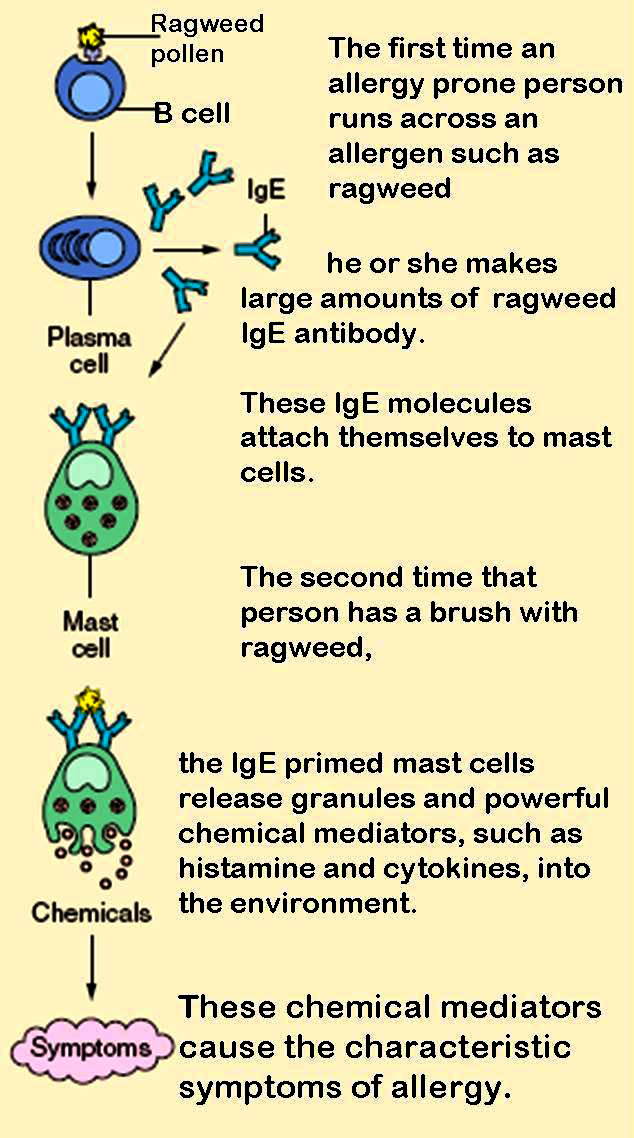
First exposure only loads the gun. Anaphylaxis is a type I (immediate) hypersensitivity reaction. The first time the immune system meets the allergen it makes IgEImmunoglobulin E, the antibody class of allergy. It coats mast cells and basophils by their tails, leaving the antigen-binding ends pointing outward like primed triggers. antibodies that clip onto high-affinity receptors on the surface of mast cells (in tissues) and basophils (in blood). The patient feels nothing. They are now sensitized, primed and waiting.
Second exposure pulls the trigger. On re-exposure the allergen bridges two adjacent IgE molecules on the mast cell surface. That cross-link is the switch. Within minutes the mast cell degranulates, releasing preformed histamine and tryptase, then synthesizing fresh leukotrienes, prostaglandin D2, and platelet-activating factor. One trigger, a flood of mediators.
Now the effects, one mediator at a time. Histamine and leukotrienes relax the smooth muscle in blood vessel walls, so vessels dilate and blood pressure falls into a vasodilatory, or distributive, shock. The same mediators make capillaries leaky, so plasma pours into tissue: that gives the hives, the lip and tongue swelling (angioedema), and it drops the blood pressure even further by emptying the vessels. In the airways, leukotrienes and histamine make bronchial smooth muscle constrict (wheeze) while the larynx swells (the stridor that closes the throat). Add cramping and vomiting from gut edema, and every system is failing on the same clock.
What pulls the trigger? The common culprits cluster by setting. Flip each card.



At the Bedside
You do not need every finding. The whole diagnosis turns on how many organ systems are firing and how fast they started after a likely trigger.
The two-system rule, in plain terms. Anaphylaxis is a clinical pattern: a sudden reaction, minutes to a few hours after exposure, hitting more than one organ system. Four systems can play, and the more you see together, the more certain you are.
When does one system alone still count? Two shortcuts complete the rule. If skin or mucosa is involved and there is either airway or blood-pressure trouble, that is enough even without a second visible system. And if a patient with a known allergen is exposed and their blood pressure drops, isolated hypotension alone is enough. The table below sorts it.
| How it qualifies | What you need to see |
|---|---|
| Pathway 1 | Sudden skin or mucosal involvement (hives, swollen lips) plus respiratory compromise OR a drop in blood pressure. No known trigger required. |
| Pathway 2 | Two or more systems after a likely allergen: skin, respiratory, cardiovascular, or persistent GI symptoms. This is the everyday two-system rule. |
| Pathway 3 | Isolated hypotension after exposure to a known allergen for that patient. One system, but the trigger is certain. |
Confirming It
Anaphylaxis is diagnosed at the bedside and treated before any test returns. One lab helps you confirm it afterward, and one mimic looks identical but laughs at epinephrine.
It is a clinical diagnosis. You never delay treatment to draw blood. That said, one test confirms mast-cell activation after the fact: serum tryptase, an enzyme stored almost exclusively in mast cells. It rises within 15 minutes, peaks around 1 to 2 hours, and falls over several hours, so you draw it during or just after the event and compare to a later baseline. Tryptase earns its keep when the diagnosis is murky or the collapse happened under anesthesia, where hives are hidden under drapes. A baseline tryptase that stays high between episodes points to mastocytosis.
Now the imposter. Picture swelling without itch, no hives, recurring for years, sometimes with attacks of belly pain, and stone-deaf to epinephrine and antihistamines. That is not anaphylaxis. That is hereditary angioedema, a deficiency of the C1-esterase inhibitorA brake on the complement and contact pathways. Without it, the enzyme that makes bradykinin runs unchecked, so bradykinin piles up and leaks fluid into deep tissue.. The swelling here is driven by bradykinin, not histamine, which is exactly why every mast-cell drug fails.
Line them up side by side. The discriminator is itch and hives plus response to epinephrine. Mast-cell swelling itches and answers epinephrine; bradykinin swelling does neither.
| Feature | Anaphylaxis | Hereditary angioedema | ACE-inhibitor angioedema |
|---|---|---|---|
| Mediator | Histamine (mast cell, IgE) | Bradykinin (low C1-inhibitor) | Bradykinin (drug-induced) |
| Itch and hives | Yes, usually | No | No |
| Onset and course | Minutes after a trigger, single event | Recurrent since youth, family history | Any time on the drug, even years in |
| Helpful lab | Tryptase rises | Low C4, low C1-inhibitor | Normal C4, history of the drug |
| Responds to epinephrine? | Yes, first-line | No | No |
| Treatment | Intramuscular epinephrine | C1-inhibitor, icatibant, ecallantide | Stop the drug; icatibant in severe cases |
The Plan
There is exactly one first move, and the board points live in why it is epinephrine and not anything else, where it goes, and what happens hours later.
Give epinephrine first, immediately. The first action in anaphylaxis is intramuscular epinephrine into the anterolateral thigh (the vastus lateralis muscle): 0.3 to 0.5 mg of the 1 mg per mL concentration in an adult, 0.01 mg per kg in a child, repeated every 5 to 15 minutes if symptoms persist. In true anaphylaxis there is no absolute contraindication. Hesitation, not epinephrine, is what kills.
Why epinephrine, and nothing else, first? Because it is the only drug that reverses every arm of the reaction at once. Read the receptors:
| Receptor | What epinephrine does | Which problem it fixes |
|---|---|---|
| Alpha-1 | Squeezes blood vessels | Raises blood pressure and shrinks airway and mucosal swelling |
| Beta-1 | Speeds and strengthens the heart | Supports cardiac output in shock |
| Beta-2 | Relaxes bronchial muscle and stabilizes mast cells | Opens the airways and shuts off further mediator release |
Why the thigh, and why intramuscular? The vastus lateralis has rich blood flow, so an intramuscular dose there reaches a high blood level fast and reliably. Subcutaneous fat absorbs slowly, and slower still when the skin is clamped down from shock, so the old subcutaneous route is out. Intravenous epinephrine is reserved for refractory shock or arrest under monitoring, because an IV bolus invites dangerous arrhythmias.
Why not antihistamines or steroids first? An antihistamine like diphenhydramine only blocks the histamine that causes itch and hives; it does nothing for airway swelling or blood pressure and works too slowly to matter in the first minutes. Steroids have no acute effect at all, since they act over hours. Both are adjuncts you give after epinephrine, never instead of it. The classic fatal error is a patient handed Benadryl while the airway closes.
Then the supporting cast. Lay the patient supine with legs elevated and keep them there; give high-flow oxygen; run a large-bore IV crystalloid bolus to refill the leaking vessels; add inhaled albuterol for stubborn wheeze. For a patient on a beta-blocker whose pressure will not climb despite epinephrine, give glucagon, which boosts the heart through a pathway that bypasses the blocked beta receptors.
It can come back: the biphasic reaction. In a minority of patients, symptoms resolve and then return 1 to 72 hours later, usually within 8 to 10 hours, with no new exposure. That is why you observe after the dust settles, commonly 4 to 6 hours and longer if the reaction was severe or needed repeat epinephrine. Discharge with two epinephrine auto-injectors, clear instructions to use them and call for help, and a referral to allergy.

