A stomach bug from two weeks ago, antibodies that mistake your own nerves for the germ, and a weakness that climbs from the feet toward the muscles that let you breathe. Learn the mimicry, the protein with no cells, the respiratory clock, and the two look-alikes that change everything.
The Setup
When Antibodies Hit the Wrong Target
Everything in this disease flows from one mistake: the immune system fights off an infection, then keeps attacking because your nerves look like the germ. Walk the chain once and the whole picture locks in.
A 32-year-old notices tingling in both feet that creeps up to his calves over two days, then his legs feel rubbery on the stairs. Two weeks earlier he had several days of bloody diarrhea after a barbecue. On exam his legs are weak on both sides and his ankle and knee reflexes are gone. Sensation is nearly normal.
What single mechanism best explains the whole story?
Start with the germ. A few weeks before the weakness, something infected the patient, most classically Campylobacter jejuni (the bloody-diarrhea bug from undercooked poultry). The immune system builds antibodies shaped to lock onto the germ. The trouble is that the sugar coat on that germ looks almost identical to the gangliosides (fatty sugar molecules) studding the myelin of your own peripheral nerves. This look-alike problem is called molecular mimicryWhen a pathogen carries a molecule so similar to a human one that antibodies built against the pathogen also bind the body. The friendly-fire mechanism behind several post-infectious diseases..
Now the attack. Those antibodies and immune cells strip the myelin (the insulating wrap that lets a nerve fire fast) off the peripheral nerves and the nerve roots where they leave the spine. A stripped segment cannot conduct → the signal slows or stops → the muscle it serves goes weak and its reflex disappears. Because the longest nerves lose insulation first, the feet and legs fail before the trunk and arms. That is why the paralysis is symmetric and ascending, and why the reflexes vanish early (areflexia).
One chain to memorize: a germ trains the immune system, the antibodies mistake nerve myelin for the germ, and the longest nerves are stripped first.
The disease has flavors. Most cases are the classic demyelinating form, but two variants show up on exams. Flip each card.
Classic AIDPTap to flip
Acute inflammatory demyelinating polyradiculoneuropathyThe usual form in North America and Europe. Myelin is the target, so nerve conduction studies show slowing and conduction block. This is the default GBS the clinical medicine describe.
Axonal AMANTap to flip
Acute motor axonal neuropathyThe antibody (often anti-GM1) attacks the axon itself rather than the myelin. Tied to Campylobacter, more common in Asia and in summer outbreaks. Pure motor, can be more severe.
Miller FisherTap to flip
The descending triadA variant marked by anti-GQ1b antibodies. The triad is eye-muscle paralysis (ophthalmoplegia), wobbly gait (ataxia), and areflexia. It starts at the head and works down, the mirror image of classic GBS.
Clinical Images
Myelin lets signals jump node to node · tap
The myelin sheath that gets stripped · tap
Campylobacter jejuni, the classic trigger · tap
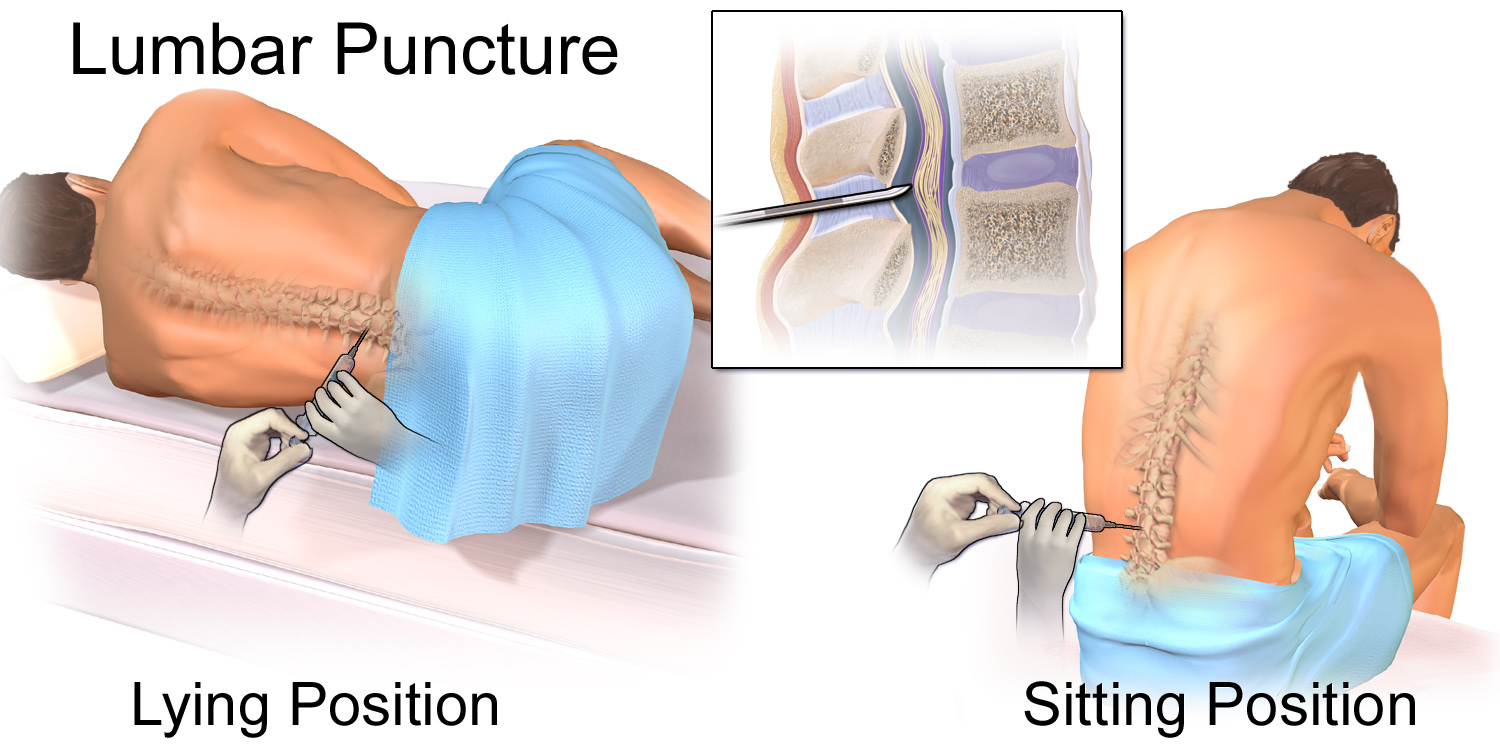
Lumbar puncture samples the fluid · tap
At the Bedside
The Pattern and the Danger
GBS follows a script: a recent infection, then a symmetric weakness that climbs while the reflexes disappear. The exam findings tell you the diagnosis, but the vital signs and the breathing tell you how scared to be.
The core picture. Over hours to a couple of weeks the patient develops symmetric weakness that starts in the legs and ascends, with areflexia (lost deep tendon reflexes) early. Tingling and numbness are common but the sensory loss stays mild compared with how weak the patient is. Progression keeps going for up to four weeks, then plateaus. A back-pain ache from inflamed nerve roots is common and can be misread as a simple strain.
Then it reaches the head and the heart. The weakness can climb to the face (often bilateral facial weakness) and the swallowing muscles (bulbar weakness, risk of aspiration). The truly dangerous parts are the diaphragm and the autonomic nervous system. Tap each feature.
Ascending weakness
Tap to reveal
Symmetric, starts distal in the legs, climbs upward. The longest nerves demyelinate first, so the feet announce the disease before the trunk.
Areflexia
Tap to reveal
Deep tendon reflexes fade or vanish, even in limbs that still have decent strength. A reflex arc cannot run through demyelinated nerve. This early loss is a signature clue.
Respiratory failure
Tap to reveal
When the weakness reaches the diaphragm, ventilation fails. Up to a third of patients need a breathing machine. This is the cause of death in GBS, so the airway is watched obsessively.
Autonomic instability
Tap to reveal
Demyelinated autonomic fibers misfire: swinging blood pressure, dangerous heart-rate changes including bradycardia and arrhythmia, ileus, and urinary retention. Sudden cardiovascular collapse is a real risk.
Bilateral facial weakness
Tap to reveal
Both sides of the face can weaken together. Two-sided facial palsy is unusual in most diseases, so it points strongly toward GBS in the right setting.
From the Attending
The patient who looks comfortable can be the one about to crash. A normal blood gas is reassuring right up until it is not, because carbon dioxide rising is a late sign of fatigue. Watch the bedside breathing numbers and the trend, not the patient comfort. The clock you are racing is the diaphragm, not the legs.
Confirming It
The Tap, the Trace, and the Mimics
The diagnosis is mostly clinical, but two tests nail it and two bedside numbers decide the ICU. Then learn the look-alikes that share the weakness but break the pattern.
The lumbar puncture. The classic finding is albuminocytologic dissociation: a high protein with a normal cell count (white cells under 10). Translate the word: high protein (albumin part) but no rise in cells (cytologic part). Inflamed roots leak protein, yet this is not a meningitis flooding the fluid with cells. The catch worth remembering: the protein is often normal in the first week, so an early tap that looks clean does not rule GBS out.
The nerve trace. Nerve conduction studies and electromyography show a demyelinating pattern: slowed conduction velocity, conduction block, and prolonged F waves (the late response that tests the nerve roots, which is where GBS strikes).
Work the decisions. Try each before you reveal it.
A patient with ascending weakness and lost reflexes after a recent diarrheal illness. Which test best supports the diagnosis?
Albuminocytologic dissociation: high protein, normal cells. Inflamed nerve roots leak protein without the cellular flood of meningitis. A head CT looks at the brain, not the peripheral nerves, and is normal here. Ascending areflexic weakness plus high-protein, low-cell fluid is GBS.
She is breathing 26 times a minute and her voice is getting softer. What bedside measure decides whether she needs the ICU and possible intubation?
Serial bedside breathing numbers catch failure early. The rule of thumb: vital capacity under about 20 mL/kg, an inspiratory force weaker than minus 30, or a drop of more than 30 percent should trigger intubation. Oxygen saturation and the blood gas fall late, after the patient is already tiring. Trend the vital capacity. Do not wait for the gas to go bad.
A different patient has weakness, but it is fatigable, started in the eyelids and double vision, and the reflexes are normal. Which is the better next test?
This is not GBS. Fatigable weakness that begins in the eyes with preserved reflexes is myasthenia gravis. You want acetylcholine receptor antibodies and a decremental response on repetitive nerve stimulation. Ocular and fatigable with intact reflexes points to the junction, not the myelin.
The two big mimics. Both make a patient weak, but each breaks the GBS pattern in a way you can name. Flip the cards, then catch the rest in the table.
Myasthenia gravisTap to flip
The fatigable junctionAntibodies block the acetylcholine receptor at the neuromuscular junction. Weakness is fatigable (worse with use, better with rest), starts in the eyes (ptosis, double vision), and reflexes are normal. No sensory loss, no antecedent diarrhea. Repetitive stimulation gives a decrement.
BotulismTap to flip
The descending blockA toxin stops acetylcholine release. Paralysis descends: it starts with the cranial nerves (double vision, drooping lids, trouble swallowing, slurred speech) and dilated, fixed pupils, then moves down. Watch for canned food in adults and honey in infants. Repetitive stimulation gives an increment.
Mimic
What separates it from GBS
Myasthenia gravis
Fatigable, ocular onset, normal reflexes, no sensory loss. Decrement on repetitive nerve stimulation.
Botulism
Descending paralysis starting in the cranial nerves, dilated fixed pupils, dry mouth and constipation. Increment on repetitive stimulation.
Tick paralysis
Ascending too, but rapid over hours and the cerebrospinal fluid is normal. Find and remove the attached tick and it resolves.
Transverse myelitis
A clear sensory level on the trunk, early bowel and bladder loss, and upper motor neuron signs. The lesion is in the cord, not the peripheral nerve.
Hypokalemic paralysis
Episodic flaccid weakness with a low serum potassium (3.5 to 5.0 normal). Reflexes return when potassium is corrected.
The Plan
Support the Breathing, Calm the Antibodies
Management is two tracks at once: protect the airway and the heart while the storm runs, and shorten the storm with immunotherapy. The single most tested point is the treatment you must not give.
Monitor first. Admit to a setting that can support breathing. Track the bedside vital capacity and inspiratory force, watch the heart rhythm and blood pressure for autonomic swings, and intubate early when the breathing numbers fall rather than waiting for a crisis.
Shorten the attack. Two treatments work and they are equally effective: intravenous immunoglobulin (a flood of pooled antibodies that distracts and dampens the immune attack) or plasma exchange (filtering the harmful antibodies out of the blood). Pick one. You do not combine them, because adding the second gives no extra benefit.
Now the trap.Corticosteroids do not help acute GBS and may even slow recovery. This is the opposite of what your instinct says for an autoimmune attack, and it is exactly why it is tested. Steroids do help the chronic cousin (chronic inflammatory demyelinating polyneuropathy) and multiple sclerosis, but not this disease.
From the Attending
When the question stem dangles high-dose steroids for a classic ascending areflexic paralysis, that is the wrong answer wearing a convincing costume. IVIG or plasma exchange, never both, and steroids do nothing here. Memorize the exception and the trap loses its teeth.
Supportive care and prognosis. Add clot prevention for immobile legs, pain control for the nerve-root ache, bladder and bowel care, and physical therapy as strength returns. Most patients recover well over weeks to months, though a minority are left with residual weakness. Recovery generally walks back down the way the weakness climbed up.
Board Trap
A patient with GBS who suddenly drops the heart rate or swings the blood pressure is showing autonomic instability, not a separate cardiac disease. Do not chase it with aggressive long-acting drugs that can overshoot when the autonomic tone flips back. Monitor closely, treat cautiously, and keep resuscitation ready. The autonomic storm is part of the disease, and it can kill as surely as the diaphragm.
Prove It
Board Walkthrough
Seven original clinical vignettes, 5 dealt per round, answer choices shuffled, never repeating within a round. Tap a wrong answer first to see why it almost works, then read the glowing clues.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.