Bugs climb a normally sterile pipe. The board game is location and host: is the bladder infected or the kidney, is the patient simple or complicated, and is this a real infection or just colonized urine you should leave alone.
The Setup
An Infection That Climbs
Almost every UTI starts the same way: gut bacteria reach the urethra, climb upward, and the higher they get, the sicker the patient. Walk the ladder once and the whole topic sorts itself.
A 24-year-old woman has two days of burning when she urinates, a constant urge to go, and pressure just above the pubic bone. She has no fever, no back pain, and no nausea. She became sexually active with a new partner last week.
Where is the infection, and what does that tell you about how sick she should look?
Start at the bottom of the ladder. The urinary tract is normally sterile above the distal urethra. Infection almost always travels the ascending route: bowel flora colonize the area around the urethra → climb into the bladder (cystitis) → and if they keep going up the ureter they reach the kidney (pyelonephritis). Women get more UTIs because the urethra is short and sits close to the anus, which is why the first UTI of a young woman after new sexual activity is so classic.
Height equals sickness. Bladder infection gives local symptoms: burning (dysuria), frequency, urgency, and suprapubic pressure, with no fever and a patient who looks well. Once bacteria invade kidney tissue you get a systemic illness: fever, chills, flank pain, costovertebral angle tenderness, nausea and vomiting. Same organisms, different floor of the building, completely different patient.
Know your bugs. One organism dominates, but the runners-up each carry a board clue. Flip each card.
E. coliTap to flip
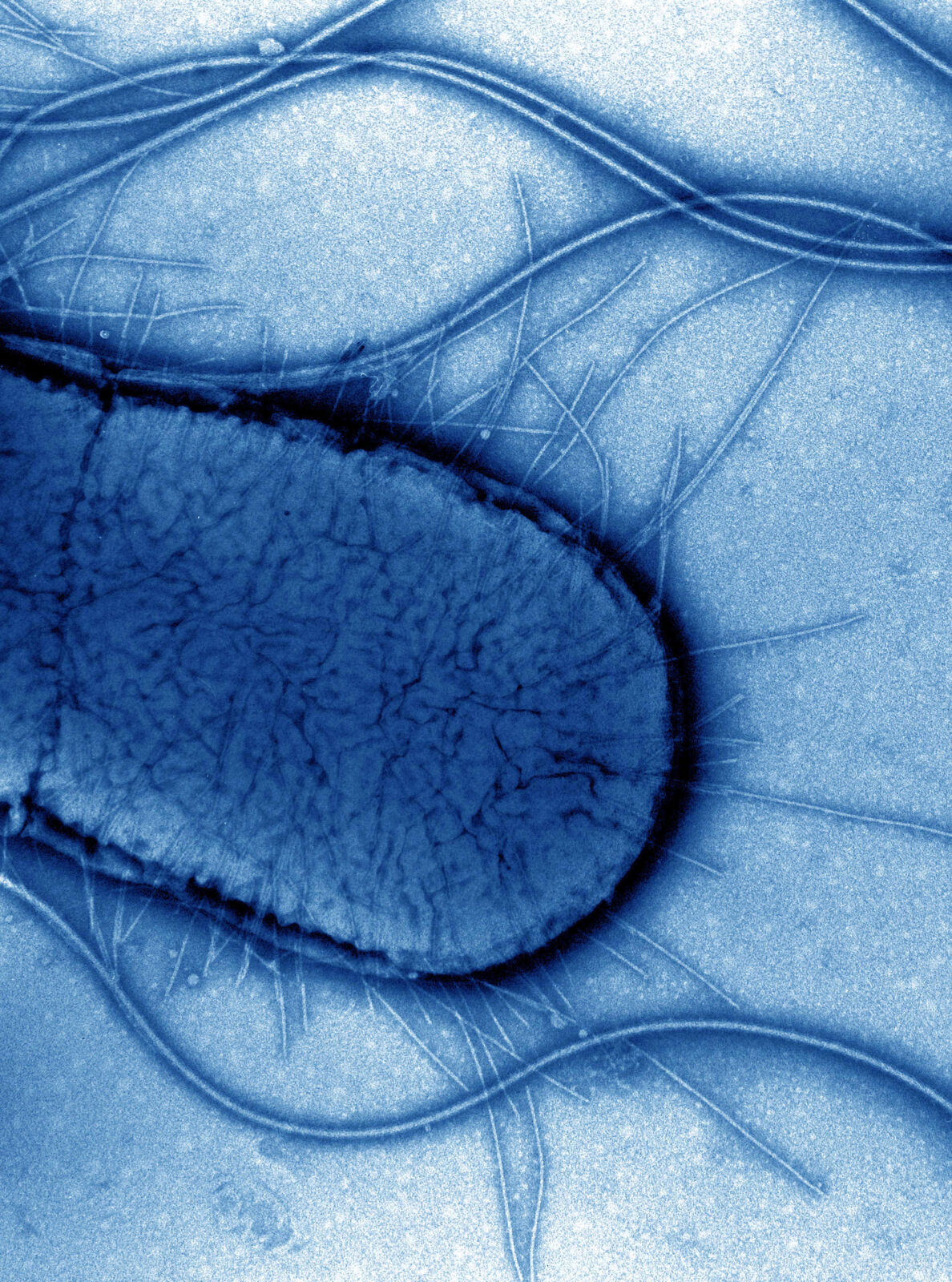
The default answerCauses roughly 80 percent of uncomplicated UTIs. A gram-negative rod that ferments lactose and turns urine nitrite positive because it reduces dietary nitrate to nitrite. If a stem gives no special clue, the bug is E. coli.
S. saprophyticusTap to flip
Young, sexually active womenA gram-positive coagulase-negative staph, novobiocin resistant. The classic second-most-common cause of cystitis in young women. It does not reduce nitrate, so the urine is often nitrite negative despite real infection.
ProteusTap to flip
Stones and alkaline urineProteus mirabilis makes urease, which splits urea into ammonia and drives urine pH up. Alkaline urine precipitates struvite (staghorn) stones. A recurrent UTI with urine pH near 8 and a staghorn calculus is Proteus.
KlebsiellaTap to flip
Also urease positiveA gram-negative rod, the third most common uropathogen, more common in hospitalized and catheterized patients. Like Proteus it can raise urine pH and form stones. Mucoid colonies from a thick capsule.
Clinical Images
E. coli, the dominant uropathogen · tap to expand
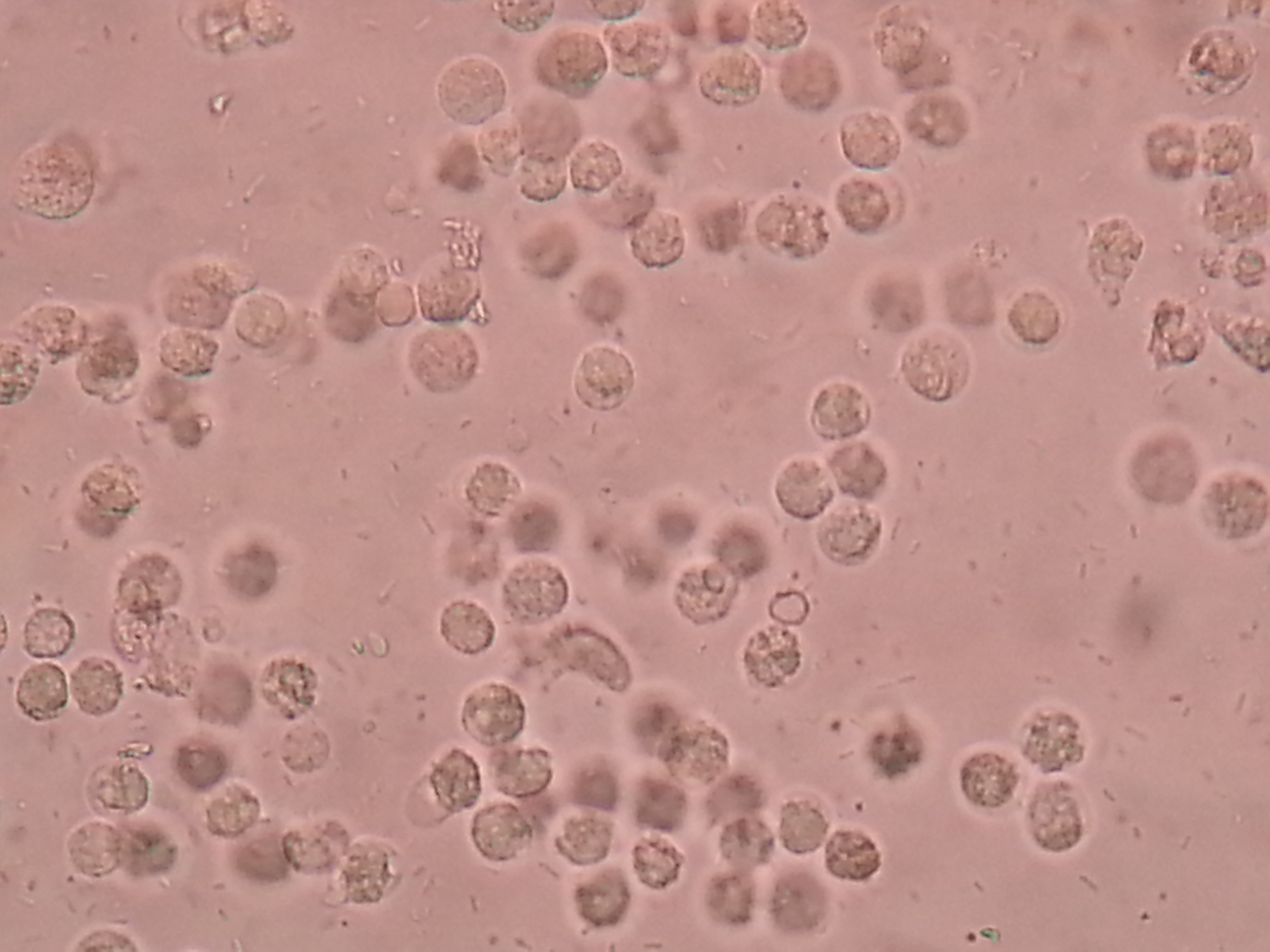
Pyuria: white cells on urine microscopy · tap
Staghorn struvite stone from urease bug · tap
At the Bedside
Simple, Complicated, and the Quiet Carriers
Two questions reshape every UTI vignette: is this host simple or complicated, and does the patient actually have symptoms or just bacteria in the urine. Get those two wrong and you treat the wrong patient.
Uncomplicated versus complicated. An uncomplicated UTI is cystitis in a healthy, non-pregnant woman with a normal urinary tract. Complicated means anything that makes the infection harder to clear or more dangerous: a man, pregnancy, a catheter, diabetes, immunosuppression, kidney stones or obstruction, a structural abnormality, or pyelonephritis itself. The label matters because complicated UTIs get cultured, get broader or longer therapy, and are more likely to be admitted.
From the Attending
A UTI in an adult man is complicated by definition. The male urethra is long, so bacteria do not climb it easily; when they do, suspect something pushing back. In an older man think prostatic obstruction, and a tender boggy prostate means prostatitis, not simple cystitis. Do not massage an acutely inflamed prostate, and treat for longer with an agent that penetrates prostate tissue.
Now the trap that sinks people: bacteria without symptoms.Asymptomatic bacteriuriaA positive urine culture (for women, two voided samples with the same organism at high count) in a patient with NO urinary symptoms and no systemic signs of infection. is common in older adults and catheterized patients, and treating it does nothing but breed resistance and cause side effects. Tap each card for who to treat and who to leave alone.
Pregnant patient
Treat or leave alone?
Treat. Untreated bacteriuria in pregnancy progresses to pyelonephritis and raises the risk of preterm birth and low birth weight. Screen with a culture at the first prenatal visit and treat a positive result even with no symptoms.
Before a urologic procedure
Treat or leave alone?
Treat. Before a procedure expected to cause mucosal bleeding (for example transurethral resection of the prostate), clear the bacteriuria first to prevent bacteremia and sepsis when the mucosa is breached.
Older adult, no symptoms
Treat or leave alone?
Leave alone. A positive culture with no urinary symptoms is colonization. Antibiotics do not help and cause harm. Mild chronic confusion at baseline without fever or new urinary symptoms is not a reason to treat.
Chronic indwelling catheter
Treat or leave alone?
Leave alone if asymptomatic. Catheters are colonized within days; a positive culture is expected. Treat only when there are true signs of infection (fever, rigors, new flank or suprapubic pain), and exchange the catheter.
Diabetic, no symptoms
Treat or leave alone?
Leave alone. Diabetes does not move a patient into the treat group for asymptomatic bacteriuria. The two exceptions stay the same: pregnancy and pre-urologic procedure.
Board Trap
A confused nursing home resident with a positive urine culture but no fever and no new urinary symptoms is the favorite trick. The reflex is to blame the urine and start antibiotics. Resist it. Look for another cause of the delirium, because treating colonized urine does not fix the patient and risks Clostridioides difficile and resistance. Only true symptoms or systemic signs justify antibiotics.
Reading the Urine
The Dipstick and the Microscope
The urinalysis is the whole workup for most UTIs. Learn what each strip pad means, the one finding that says kidney, and when a clean-looking dipstick is actually hiding something else.
Two strip pads do the heavy lifting.Leukocyte esterase is an enzyme released by white blood cells; a positive pad means pyuria (white cells in the urine), the marker of inflammation. Nitrites turn positive when bacteria reduce dietary nitrate to nitrite, which only the gram-negative Enterobacteriaceae like E. coli do well. So a positive nitrite is fairly specific for a gram-negative bug, but a negative nitrite does not exclude UTI: Staphylococcus saprophyticus and Enterococcus do not make nitrite.
One finding localizes to the kidney. Both cystitis and pyelonephritis show pyuria and bacteriuria. The discriminator is the white blood cell cast, a cylinder of white cells molded in a renal tubule. Casts can only form upstream in the nephron, so a white blood cell cast plus fever and flank pain equals pyelonephritis, not cystitis.
Work the algorithm. Try each fork before you reveal it.
A healthy 25-year-old woman with classic dysuria and frequency, no fever, no flank pain. What workup does she need before treatment?
For uncomplicated cystitis the diagnosis is clinical plus a dipstick. You treat empirically and do not need a culture or imaging. Simple cystitis in a healthy woman: dipstick, then treat. No culture required.
A 30-year-old woman with fever to 102 F, flank pain, and vomiting. Urinalysis shows pyuria and a white blood cell cast. What does the cast tell you?
White blood cell casts form only in the renal tubules, so they place the infection in the kidney. With fever and flank pain this is pyelonephritis, a complicated UTI that earns a culture and often imaging. White blood cell casts equal upper-tract disease.
A sexually active 22-year-old woman with dysuria. Urinalysis shows pyuria but the culture grows nothing and nitrites are negative. Best next step?
Pyuria with a sterile routine culture is sterile pyuria. In a young sexually active patient think urethritis from chlamydia or gonorrhea; other causes include tuberculosis and recently treated UTI. Pyuria plus negative culture: hunt for chlamydia, gonorrhea, or TB.
From the Attending
A few squamous epithelial cells and mixed organisms on a urinalysis usually mean a contaminated sample, not infection. Before you commit to a diagnosis, ask whether the specimen was a clean catch. A repeat clean catch or a straight catheter sample beats treating skin and vaginal flora as a pathogen.
The Plan
Matching the Antibiotic to the Patient
Empiric therapy is not one drug. It changes with location and host: simple cystitis, full-blown pyelonephritis, and pregnancy each have their own short list, and a couple of drugs carry hard rules about where they can and cannot go.
Uncomplicated cystitis. First-line is one of three: nitrofurantoin for 5 days, trimethoprim-sulfamethoxazole for 3 days where local resistance is low, or a single dose of fosfomycin. Save fluoroquinolones for when these cannot be used, because their collateral damage (tendon rupture, C. difficile, resistance) is too high a price for a simple bladder infection.
Pyelonephritis. A kidney infection needs a drug that reaches kidney tissue and blood. A stable outpatient can take an oral fluoroquinolone, often after a single dose of intravenous ceftriaxone. Admit and give intravenous antibiotics when the patient is septic, vomiting and cannot keep pills down, pregnant, or failing outpatient care.
Board TrapNitrofurantoin does not treat pyelonephritis. It concentrates in the urine but never reaches useful levels in kidney tissue or blood, so it works for cystitis only. It also needs decent kidney function and is avoided when creatinine clearance is low. Pick nitrofurantoin for the bladder, never for the febrile flank-pain patient.
Pregnancy rewrites the drug list. You still treat (including asymptomatic bacteriuria), but the safe agents shift by trimester. Tap each card.
Cephalexin, amoxicillin-clavulanate
Safe in pregnancy?
Yes, broadly safe. Beta-lactams are the workhorse for UTI in pregnancy across all trimesters. Cephalexin is a common first choice for cystitis and asymptomatic bacteriuria.
Nitrofurantoin
Safe in pregnancy?
Usable in the second trimester, avoided near term. At term it can trigger hemolytic anemia in the newborn (and in mothers with G6PD deficiency). Also avoid in the first trimester when alternatives exist.
Trimethoprim-sulfamethoxazole
Safe in pregnancy?
Avoid first trimester and near term. Trimethoprim is a folate antagonist linked to neural tube defects early; the sulfa component displaces bilirubin and risks kernicterus near delivery. Reserved for mid-pregnancy when nothing else fits.
Fluoroquinolones
Safe in pregnancy?
Avoid. Linked to fetal cartilage and tendon toxicity. Not a routine choice for UTI in pregnancy; use a beta-lactam instead, and admit for intravenous therapy if pyelonephritis develops.
Feature
Cystitis
Pyelonephritis
Symptoms
Dysuria, frequency, urgency, suprapubic pressure; no fever
Nitrofurantoin, trimethoprim-sulfamethoxazole, or fosfomycin
Fluoroquinolone or ceftriaxone; intravenous if sick
Disposition
Outpatient, oral
Outpatient if stable; admit if septic, vomiting, or pregnant
Board Trap
A patient with pyelonephritis who stays febrile after 48 to 72 hours of appropriate antibiotics has not failed the drug; something is blocking the cure. Get a CT of the abdomen and pelvis to look for an obstructing stone or a perinephric or renal abscess. A blocked, infected kidney needs drainage or stone relief, not just a different antibiotic.
Prove It
Board Walkthrough
Seven original clinical vignettes, 5 dealt per round, answer choices shuffled, never repeating within a round. Tap a wrong answer first to see why it almost works, then read the glowing clues.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.