Every cough stem becomes manageable when you sort three things first: x-ray pattern, patient setting, and the one clue that names the organism.
Patternlobar, patchy, interstitial, ground-glass
SettingCAP, aspiration, HAP, VAP, HIV
Moveorganism, test, drug, escalation
First decision
Do not name the bug first. Classify the pneumonia first.
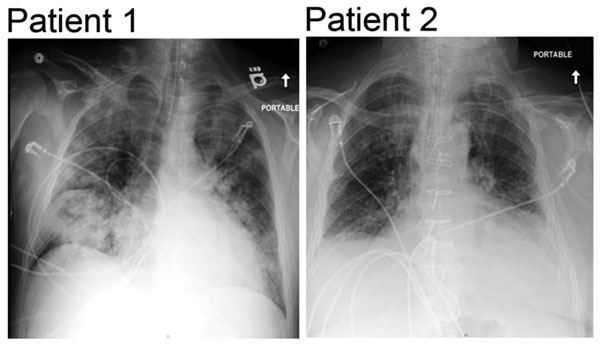
A 24-year-old military recruit presents to urgent care with ten days of dry cough, headache, and low-grade fever. He looks comfortable, but chest x-ray shows diffuse bilateral interstitial infiltrates.
Young adult in close quarters + dry cough + interstitial infiltrates + patient looks better than the film = Mycoplasma pattern. The next move is macrolide, doxycycline, or fluoroquinolone because beta-lactams need a cell wall target.
Film pattern: one dense lobe, patchy bronchial spread, or diffuse interstitial haze.Diplococci plus lobar consolidation locks pneumococcus.Alveolar exudate gives consolidation. Interstitial wall inflammation gives haze.
Pattern and pathogen
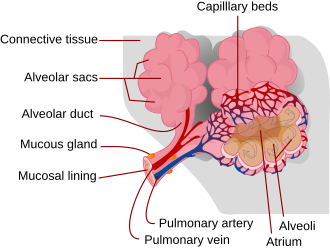
The first split is loud alveoli versus quiet interstitium.
Typical pneumonia fills alveoli with exudate, so the patient looks sick and the film consolidates. Atypical pneumonia inflames the interstitial wall, so the cough is dry and the film can look worse than the bedside.
Typical pattern
Sudden onset with fever, rigors, pleuritic pain, and productive cough.
Lobar consolidation means alveoli are full of inflammatory exudate.
Classic culprit: Streptococcus pneumoniae, especially with rusty sputum and gram-positive diplococci.
Other signatures: Klebsiella with currant jelly sputum, Staph aureus after influenza, H. influenzae in COPD.
Atypical pattern
Gradual onset with dry cough, headache, malaise, and lower fever.
Diffuse interstitial infiltrates come from alveolar wall inflammation, not pus filling one lobe.
Classic culprit: Mycoplasma in young adults, close quarters, and cold agglutinins.
Water plus GI symptoms: Legionella until proven otherwise, especially with hyponatremia.
Rusty sputum, sudden fever, rigors, pleuritic pain, lobar consolidation, gram-positive lancet-shaped diplococci. It stays the default unless the stem gives a stronger named clue.
MycoplasmaWalking pneumonia
Young adult, school or military setting, dry cough, interstitial infiltrates, x-ray worse than the patient, cold agglutinins. No cell wall means beta-lactams miss.
KlebsiellaNecrotizing alcohol clue
Alcohol use or diabetes, thick bloody mucoid sputum, upper-lobe cavitation, gram-negative rod with capsule. Currant jelly is the override clue.
LegionellaWater plus gut
Hotel, cruise, air conditioner, or water aerosol exposure with pneumonia plus diarrhea, confusion, high fever, and hyponatremia. Urinary antigen is the fast test.
S. aureusPost-flu crash
Influenza damages the airway, the patient improves, then returns with sudden severe fever and cavitary infiltrates. Gram-positive cocci in clusters point here.
PseudomonasVentilator and CF
Think ventilator, late hospital course, cystic fibrosis adult, bronchiectasis, severe structural lung disease, green sputum, or oxidase-positive gram-negative rod.
PneumocystisCD4 threshold
HIV with CD4 below 200, subacute dyspnea, dry cough, elevated LDH, bilateral ground-glass opacities. Treat with TMP-SMX and add steroids for severe hypoxemia.
Aspiration floraDependent lobe
Seizure, dysphagia, altered consciousness, stroke, or anesthesia plus dependent infiltrate. Oral anaerobes dominate; nursing home and hospital settings add gram-negative rods.
Setting to treatment
The drug choice follows the room the patient is in.
Outpatient CAP, inpatient CAP, ICU CAP, aspiration, hospital-acquired pneumonia, and ventilator-associated pneumonia are different ecosystems. The mistake is treating them like the same cough.
Community-acquired pneumonia
Healthy outpatient: amoxicillin or doxycycline. Macrolide only when local resistance is low.
Comorbid outpatient: respiratory fluoroquinolone, or beta-lactam plus macrolide.
Inpatient floor: ceftriaxone plus azithromycin, or respiratory fluoroquinolone.
Move: inpatient CAP coverage. Use ceftriaxone plus azithromycin, or a respiratory fluoroquinolone. The beta-lactam hits typical organisms; the macrolide covers atypicals.
Aspiration and immunocompromise
Aspiration: dependent lobe plus risk for impaired swallow or consciousness.
Severe PCP hypoxemia: TMP-SMX plus corticosteroids.
Move: PCP treatment. Use TMP-SMX. Add corticosteroids when PaO2 is below 70 mm Hg or A-a gradient is high, because inflammation worsens oxygenation during therapy.
Hospital and ventilator pneumonia
HAP starts after 48 hours in the hospital.
VAP starts after 48 hours on the ventilator.
Late VAP and severe HAP need Pseudomonas and MRSA coverage while cultures are pending.
Move: late VAP coverage. Use an antipseudomonal beta-lactam plus a second antipseudomonal agent and add vancomycin or linezolid for MRSA risk, then narrow with cultures.
Bedside lock
Consolidation increases tactile fremitus and bronchial breath sounds because sound travels better through fluid-filled alveoli than through air. That finding belongs with lobar bacterial pneumonia, not pure bronchospasm.
Clinical walkthrough
Thirty-four bedside cases, shuffled, one at a time.
Commit to the organism, test, or drug. After you answer, the clue text lights up and the explanation walks the discrimination without dumping a wall of prose.
Case 1 of 34Pattern
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.