Stack triggers to push the patient toward an AIP attack. Watch the severity bar rise, symptoms light up. Apply the right treatments to bring it down.
Patient · Quiet at baseline
Each trigger induces hepatic ALA synthase. Stack enough and the partial PBG deaminase block becomes a clinical attack. Treatments bypass the trigger or shut down ALA synthase directly.
Attack severityQuiet
Add a trigger
Symptoms (light up as severity climbs)
Vague abdominal pain
Severe colicky pain + nausea
Dark / port-wine urine
Tachycardia + HTN (autonomic)
Motor weakness, neuropathy
Anxiety, hallucinations, seizures
Respiratory paralysis (crisis)
Treatments (subtract from severity)
No events yet.
From the Attending
AIP is a setup, not a constant. Patient is fine until the liver gets pushed to make more heme · sulfa / barbiturate / OCP / fasting / alcohol / infection / smoking induce ALA synthase. PBG deaminase can\'t keep up · ALA + porphobilinogen pile up · the nervous system gets toxic. Treat in this order: stop the trigger, IV glucose (turns off ALA synthase upstream), then IV hemin (negative feedback at ALA synthase). Don\'t treat porphyria with phenobarb · you\'ll make it worse.
BIOCHEM · Heme Synthesis
Acute Intermittent Porphyria
Trigger opens the faucet. PBG deaminase blocks the pipe. ALA/PBG spill out, and the patient gets NEUROVISCERAL.
Here is your patient: A 24-year-old woman has severe cramping abdominal pain, constipation, anxiety, and reddish urine after starting an antiseizure drug. Her abdomen is tender but has no rebound or guarding. Which enzyme is most likely deficient?
Ferrochelatase
Porphobilinogen deaminase
Uroporphyrinogen decarboxylase
Glucose-6-phosphate dehydrogenase
The clue is not just dark urine. It is dark urine plus neurovisceral chaos: abdominal pain, constipation, anxiety, neuropathy, tachycardia, or hypertension after a trigger. A trigger raises hepatic heme demand, ALA synthase opens the faucet, and the blocked PBG deaminase step makes ALA/PBG pile up. Those precursors irritate nerves. AIP = PBG deaminase deficiency = abdominal pain + psych/autonomic symptoms + dark urine.
1 / 7
The Heme Factory
Run the trigger. Watch the blocked assembly line spill neurotoxic precursors.
Chapter I · Hector Idles
HECTOR
"Hector the hepatocyte is quiet. ALA synthase idles. PBG deaminase is narrow, but nothing is overflowing yet."
Baseline: Hector makes heme calmly. ALA becomes PBG, PBG moves downstream, and finished heme keeps the faucet quiet.
Chapter II · Hector Gets Pushed
ALA SYNTHASE UP
"Barbiturate, alcohol, fasting, hormones. Liver demands more heme."
A trigger tells Hector to make more heme. He opens the ALA synthase faucet, so more raw material rushes into the line.
Chapter III · Hector Overflows
PBG DEAMINASE BLOCK
"PBG cannot clear. ALA/PBG back up and spill into nerves and urine."
Now the chain becomes clinical: more inflow meets the PBG deaminase block, ALA/PBG back up, and the spill irritates nerves.
Pattern Locked · AIP
The AIP Chain
RouteTrigger → ALA synthase up → PBG deaminase block → ALA/PBG accumulate → nerves irritated
PearlSevere abdominal pain with a quiet exam is wiring pain, not peritoneal fire.
🎯Board clue chain: high porphyrin precursors, urine δ-ALA and porphobilinogen, then abdominal pain, neuropathy, and red-dark urine.
✓Move: stop the trigger, then give glucose and hemin to turn down ALA synthase upstream.
⚠Board trap: dark urine after a drug can look like G6PD, but G6PD gives hemolysis signs. AIP gives nerve signs.
From the Attending
Heme synthesis is the playground for the porphyrias. ALA synthase (mitochondria) is the rate-limiter, induced by anything that depletes hepatic heme: alcohol, sulfa, antifungals, OCPs, smoking, fasting, infection. PBG deaminase (cytosol) is broken in AIP · ALA + porphobilinogen pile up · both are neurotoxic, neither photosensitizes the skin (no porphyrins past this block). That's why AIP gives abdominal pain + neuropathy + psychiatric symptoms but NEVER photosensitivity. Porphyria cutanea tarda blocks LATER in the pathway (uroporphyrinogen decarboxylase) → porphyrins build up → sun-exposed skin blisters. Position in the pathway predicts the symptom set.
Trigger Lab
Change the state. Watch what raises precursor pressure and what shuts the faucet back down.
Attack Console
Idle pressure
Baseline: the pathway is narrow but quiet. ALA synthase is not being pushed, so the PBG deaminase block is not yet overflowing.
triggerALA synthasePBG blocknerve spilltreat
The Triad Lineup
Tap a card. Front: the clue. Back: why that clue belongs to the same blocked factory.
From the Attending
The AIP "5 P" mnemonic: Painful abdomen, Polyneuropathy, Psychological, Pink-port-wine urine, Precipitated by drugs/fasting/EtOH. Young woman 20·40 with recurrent episodes of vague abdominal pain that gets a normal CT and a clean exam, plus weakness or paresthesias and dark urine after starting a new drug · that's the AIP vignette. Confirm with urinary porphobilinogen during an attack (high). Treat the attack: stop the trigger, give IV glucose (turns off ALA synthase), then hemin (negative feedback at ALA synthase). clinical medicine may show urine that turns dark or red on standing · PBG converts to porphobilin on light/air exposure.
Abdominal Pain
Autonomic nerves · Silent abdomen
FeelSevere cramping, constipation, no peritoneal signs
TrapLooks surgical, exam stays quiet
Pain without peritonitis = nerves, not knife
tap to flip →
Why The Belly Hurts
Trace It
ALA/PBG irritate autonomic nerves. The bowel wiring is angry, so the patient feels brutal pain and constipation even though the peritoneum is not inflamed.
Lock It
Severe belly pain with a quiet abdominal exam is the AIP doorbell.
Psych / Neuro
Brain and peripheral nerves
FeelAnxiety, hallucinations, seizures, neuropathy
TrapLooks psychiatric until the urine and belly clues arrive
Psych plus belly pain is not primary psych
tap to flip →
Why The Mind Changes
Trace It
The same precursor spill irritating gut nerves can irritate CNS and peripheral nerves. That turns one pathway problem into a mixed psych-neuro stem.
Lock It
Pattern, not fragment: psych symptoms + severe abdominal pain + dark urine = AIP until proven otherwise.
Dark Urine
Precursor spill · Oxidation
FeelTea-colored or reddish urine after standing
TrapCan bait hemolysis if you ignore neurovisceral signs
Dark urine seals the pathway story
tap to flip →
Why The Urine Darkens
Trace It
ALA/PBG and porphyrin precursors leave through urine. Air and light oxidize the spill, so the urine darkens after standing.
Lock It
Dark urine plus neurovisceral symptoms = porphyria until proven otherwise.
Trap Lab
AIP is a pattern diagnosis. Kill the distractors by asking what system is actually failing.
1
The belly pain is severe. What keeps AIP alive?
The pain is real, but the peritoneum is not inflamed. AIP hurts through autonomic neuropathy, so the stem gives severe colicky pain, constipation, tachycardia, and a soft abdomen instead of rebound or guarding.
2
Which companion clue points away from G6PD?
G6PD breaks red cells, so expect jaundice, bite cells, and oxidant exposure. AIP poisons nerves and spills heme precursors into urine, so the winning cluster is belly pain + psych/autonomic findings + darkening urine.
3
What is the treatment logic?
Hemin restores the missing end product and represses hepatic ALA synthase; glucose also suppresses ALA synthase expression. Both reduce fresh precursor buildup rather than just treating symptoms.
See It In Real Patients
Tap any image to expand. These are the visual anchors clinical medicine test.
Porphyria Urine Darkens after standing as ALA/PBG oxidize. The classic port-wine color.
PCT Blistering Sun-exposed hands in porphyria cutanea tarda. Skin-first, not nerve-first.
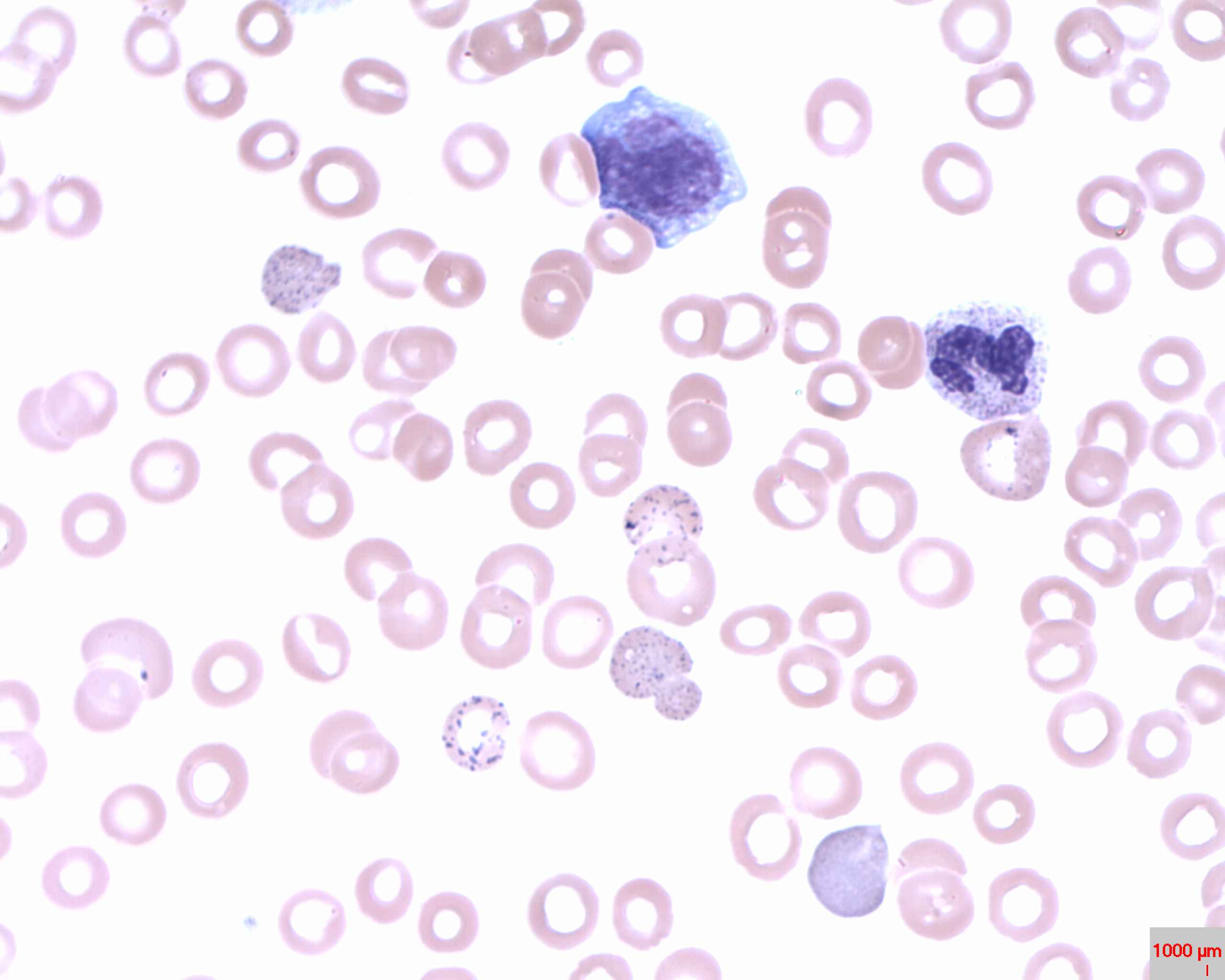
Basophilic Stippling Lead inhibits ALA dehydratase and ferrochelatase. Same pathway, different block.
Heme Biosynthesis Full pathway from glycine + succinyl-CoA to heme. AIP blocks step 3 (PBG deaminase).
Board Challenge
Original AIP stems. The explanations eliminate the traps.
From the Attending
Don't anchor on the abdomen. clinical medicine reward you for picking the diagnosis when the surgical workup is negative. "Recurrent severe abdominal pain + normal imaging + autonomic neuropathy + dark urine + new drug exposure" is AIP · not appendicitis, not endometriosis, not IBS. "Photosensitive blistering rash + dark urine + EtOH/HCV" is porphyria cutanea tarda. "Microcytic anemia + basophilic stippling + abdominal pain + neuropathy in a child" is lead poisoning (lead inhibits ALA dehydratase AND ferrochelatase · same pathway, different block). Same pathway diagram explains 80% of the porphyria board pool.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.