Hemolytic Anemias
When RBCs are destroyed faster than they can be replaced
Clinical Images
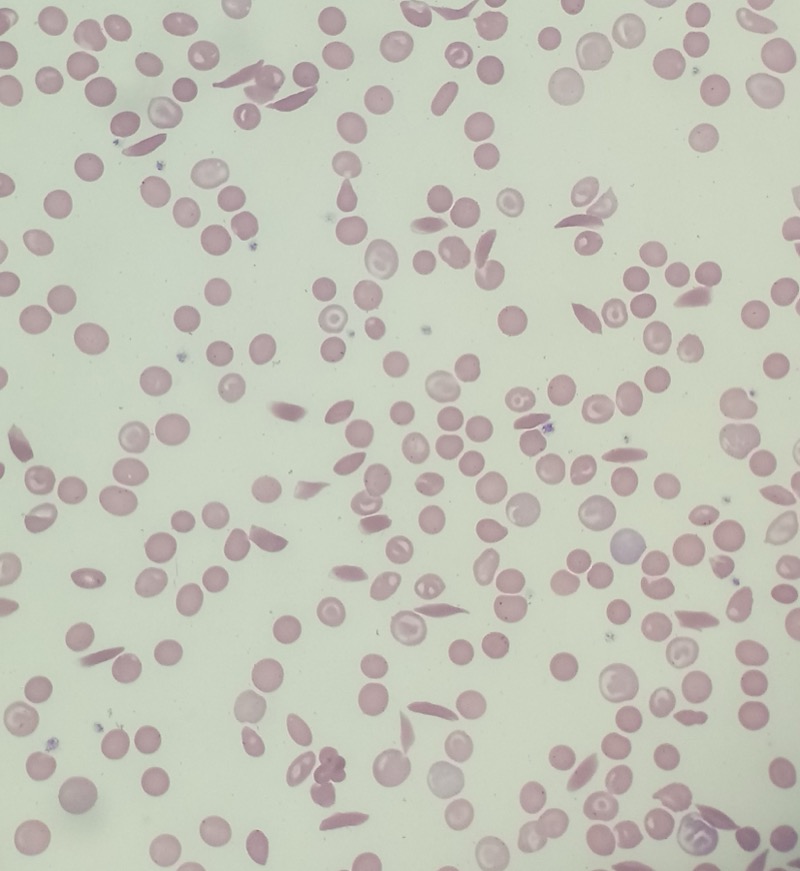




🚨 Clinical Vignette
A 28-year-old woman presents with fatigue, jaundice, and dark urine. Labs show Hgb 8.2, elevated retic count (15%), and unconjugated hyperbilirubinemia. Her direct Coombs test is positive. There are no schistocytes on blood smear.
What type of hemolysis is occurring?
The Players: Globin, Haptoglobin & the Hb Family
Before the hemolysis labs make sense, know who's in the room. Globin lives inside the RBC. Haptoglobin patrols plasma. And not all hemoglobins are the same.
| Name | Chains | Board Pearl |
|---|---|---|
| HbA | α2β2 | Normal adult Hb. The Goal. |
| HbF | α2γ2 | Fetal. Higher O2 affinity. Hydroxyurea raises it. |
| HbA2 | α2δ2 | Elevated in beta-thalassemia (>3.5%). |
| HbS | α2βS2 | Sickle cell. Valine for glutamate at β6. Sticky when deoxygenated. |
| HbC | α2βC2 | Lysine for glutamate at β6. Ly-C-ne mnemonic. |
| HbH | β4 | Alpha-thal (3 gene loss). H = Heinz bodies · beta tetramers precipitate. |
| Hb Barts | γ4 | Alpha-thal (4 gene loss). Lethal · hydrops fetalis. |
Tap the blurred answer. Tap again for the next beat.
| Lab | Thalassemia Blueprint |
IDA Ingredients |
|---|---|---|
| Ferritin | Normal / High | Low · #1 early marker |
| TIBC | Normal | High (liver hunting for iron) |
| RDW | Normal (uniformly small) | High (mixed sizes) |
| RBC Count | High (compensatory) | Low / Normal |
| Mentzer Index | <13 suggests thal | >13 suggests IDA |
Thalassemia (Blueprint)
IDA (Ingredients)
| Lab | Thal MINOR Trait |
Thal MAJOR |
|---|---|---|
| RDW | Normal (uniformly small) | High (fragments everywhere) |
| RBC Count | High (compensatory) | Low (marrow failure + hemolysis) |
| Hemoglobin | Mild anemia (10-12) | Severe (<7) |
| Clinical | Asymptomatic / mild fatigue | Transfusion dependent |
Thal MINOR (Trait)
Thal MAJOR
The Big Picture: Reticulocytosis = Hemolytic Anemia
A high reticulocyte count screams hemolytic anemia. It's NOT a bone marrow problem. The bone marrow is overproducing because red blood cells are being destroyed faster than normal in the periphery.
Hemolysis is one lab tuple and two questions.
Normal RBC lifespan: 120 days
In hemolytic anemias: days to weeks
The bone marrow responds by:
• Releasing immature RBCs (reticulocytes) before they're fully mature
• Increasing RBC production up to 6-8x normal
• This hyperproliferation = elevated reticulocyte count
Which Diseases Cause Which Type?
Primarily Extravascular:
Hereditary Spherocytosis → osmotic fragility, bursts in hypotonic saline
Hereditary Elliptocytosis → structural RBC defect
Sickle Cell Disease → vaso-occlusion + splenic infarction
HbC Disease → RBC damage
Pyruvate Kinase Deficiency → RBC fragility
Warm Agglutinin Hemolytic Anemia (IgG antibodies, positive direct Coombs)
Intravascular + Extravascular (Both):
G6PD Deficiency → oxidative stress + hemolysis in oxidative crises
Cold Agglutinin Disease → IgM-mediated
Primarily Intravascular:
PNH → complement-mediated
Microangiopathic Hemolytic Anemia (MAHA) → TTP, HUS, DIC
Malaria → parasite destruction
Board Walkthrough
25 original clinical vignettes. One at a time, shuffled, never repeats. Right-click or long-press to cross out. Double-tap to highlight.