📷 CSF: cloudy/purulent in bacterial meningitis · tap to expand
📷 Petechial rash: non-blanching · think meningococcus · tap to expand
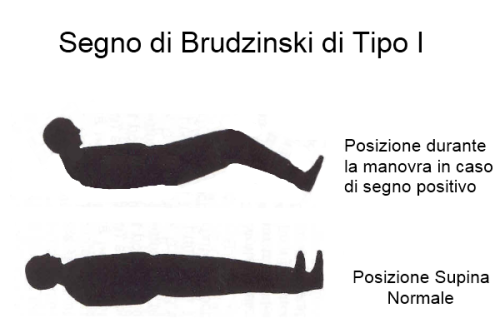
📷 Brudzinski sign: neck flexion causes hip flexion · tap to expand
Meningitis
Bacterial vs viral vs fungal. CSF patterns. Age-based bugs. The LP decision. Everything clinical medicine throws at you about inflamed meninges.
Opening Case
A 19-year-old college student presents with high fever, neck stiffness, and a petechial rash spreading across his trunk. His roommate had similar symptoms last week. What's the most likely organism?
Textbook N. meningitidis. College dorm + petechiae + close-contact spread = meningococcal meningitis. The rash is the giveaway · it's the only common meningitis bug that causes petechiae/purpura from endotoxin-mediated vascular damage.
Good thinking, but the petechial rash + college dorm setting screams N. meningitidis. S. pneumoniae is the #1 cause in adults overall, but it doesn't cause petechiae. Listeria hits the extremes of age. H. influenzae is mostly in unvaccinated kids.
SECTION 01
The Bugs · Sorted by Age
THE CLUE: clinical medicine hand you an age. That age tells you which bug colonized the meninges.
Beat 1: Neonate or elderly? → weak T-cells → Listeria can survive inside macrophages → add ampicillin.
Beat 2: College dorm or military barracks? → droplet spread → petechiae → N. meningitidis.
Beat 3: Everyone else? → S. pneumoniae is still #1 in adults.
Age bracket → organism → empiric coverage. Miss Listeria in the extremes and you lose the patient.
This is THE high-yield table for meningitis. clinical medicine will give you an age and expect you to know the bugs. Every. Single. Time.
Key Pattern
The pattern: Neonates and elderly share ListeriaListeria monocytogenes · gram-positive rod. Lives in deli meats, soft cheeses, unpasteurized milk. It's an intracellular parasite that can cross the blood-brain barrier. The reason it hits neonates and elderly: both have weak cell-mediated immunity, and Listeria requires T-cells to clear it.. Everyone in between gets S. pneumoniaeStreptococcus pneumoniae · gram-positive diplococcus, lancet-shaped. #1 cause of bacterial meningitis in adults. Also #1 cause of otitis media, sinusitis, and community-acquired pneumonia. It's the king of upper respiratory infections.. The young and crowded get N. meningitidisNeisseria meningitidis · gram-negative diplococcus (kidney-bean shaped). Transmitted by respiratory droplets. Causes outbreaks in close quarters · dorms, military barracks. Capsular serotypes B, C, Y, W most common. Only meningitis bug that causes petechial/purpuric rash and Waterhouse-Friderichsen syndrome..
🔑Listeria loves the Limits of life · neonates and elderly. The extremes.
▸
Neonates (0-3 months)
1. Group B Strep (S. agalactiae) · #1 in neonates. Mom carries it in vaginal flora, baby picks it up during delivery. 2. E. coli · gram-negative rod. K1 capsule serotype crosses the BBB. 3. Listeria monocytogenes · the deli meat killer. Weak neonatal T-cell immunity can't clear it.
1. N. meningitidis · especially in adolescents/college freshmen. Close quarters + droplet spread. 2. S. pneumoniae · still common. Unvaccinated kids at higher risk. 3. H. influenzae type b · rare now thanks to Hib vaccine. Still shows up in unvaccinated kids.
Elderly & Immunocompromised (>50 or impaired cell-mediated immunity)
1. S. pneumoniae · still #1. 2. Listeria monocytogenes · it's back! Weak T-cells can't contain it. 3. N. meningitidis · less common but still possible. 4. Gram-negative rods · E. coli, Klebsiella in the very old/debilitated.
Empiric Tx: Vancomycin + ceftriaxone + ampicillin (+ dexamethasone). The extra ampicillin covers Listeria. If you forget the ampicillin in an elderly patient, you've killed them.
Board Trap
When do you add ampicillin? Neonates (<3 months) and elderly/immunocompromised (>50). Both groups need Listeria coverage. Ceftriaxone does NOT cover Listeria. This is the single most tested meningitis treatment question in clinical practice.
🔑Ampicillin for the Aged and the Arriving (newborns). Both ends of the timeline.
A 68-year-old man with diabetes presents with meningitis. His empiric antibiotics should include vancomycin, ceftriaxone, and what additional drug?
Yes. Ampicillin covers Listeria, which ceftriaxone misses. Age >50 + immunocompromised = add ampicillin. Always.
Not quite. The key here is Listeria coverage. At 68 with diabetes, his cell-mediated immunity is weakened. Ampicillin is the only option that covers Listeria. Ceftriaxone doesn't touch it.
SECTION 02
CSF Analysis · The Pattern Recognition
They hand you CSF values. You tell them bacterial vs viral vs fungal. This is pure pattern recognition · and it's on every single practice exam.
Bacterial
Appearance: Cloudy / purulent
Opening pressure: ↑↑↑ Elevated
WBCs: ↑↑↑ Neutrophils
Protein: ↑↑ Elevated
Glucose: ↓↓ LOW
Viral
Appearance: Clear
Opening pressure: Normal / mildly ↑
WBCs: ↑ Lymphocytes
Protein: Normal / mildly ↑
Glucose: Normal
Fungal / TB
Appearance: Clear
Opening pressure: ↑↑ Elevated
WBCs: ↑ Lymphocytes
Protein: ↑↑ Elevated
Glucose: ↓↓ LOW
Tap each card · flip to see the CSF chain
💥
Bacterial
Cloudy CSF · bugs eat sugar
The Chain
Clue: Purulent/cloudy fluid.
Bacteria invade CSF → neutrophils flood in → bacteria metabolize glucose → protein leaks from inflamed meninges.
Neutrophils + low glucose = bacterial until proven otherwise.
💧
Viral
Clear CSF · sugar stays normal
The Chain
Clue: Clear fluid, patient still miserable.
Virus hijacks cells → lymphocytes respond → mild protein rise → glucose untouched (viruses do not eat CSF sugar).
Lymphocytes + normal glucose = viral pattern.
🍄
Fungal / TB
Clear CSF · sugar crashes anyway
The Chain
Clue: Looks viral on appearance but glucose is low.
Slow-growing organism → lymphocytic response → chronic protein leak → glucose consumed over days to weeks.
Bacterial & fungal: Low glucose. Bacteria and fungi eat sugar. They're metabolically active in the CSF. Viral: Normal glucose. Viruses hijack host cells to replicate · they don't consume glucose directly.
Then look at cells: Neutrophils = bacterial. Neutrophils are the first responders to bacterial infection. Lymphocytes = viral OR fungal/TB. Both are lymphocyte-predominant, but fungal/TB has LOW glucose (viral doesn't).
Board Trap
Early viral meningitis can show neutrophils. In the first 24-48 hours, viral meningitis may have a neutrophil-predominant CSF. If they give you a "repeat LP 24 hours later shows lymphocyte shift" · that's the classic viral pattern. Don't be fooled by early neutrophils into treating for bacterial when the glucose is normal.
CSF shows: lymphocytic pleocytosis, elevated protein, and low glucose. The appearance is clear. Which category?
Exactly. Lymphocytes + low glucose = fungal or TB. Bacterial would have neutrophils. Viral would have normal glucose. This pattern is fungal/TB territory · think Cryptococcus in an HIV patient or TB meningitis.
Close, but check the cells AND glucose together. Lymphocytes rules out bacterial (that would be neutrophils). Low glucose rules out viral (viral glucose is normal). That leaves fungal/TB · lymphocytes + low glucose is their signature.
SECTION 03
Signs, Complications & Emergencies
The classic triad: fever, neck stiffness, altered mental status. But clinical medicine loves the specific signs.
Sign
What It Is
What It Means
Kernig sign
Patient supine, hip and knee flexed to 90°. Try to extend the knee → resistance and pain
Meningeal irritation. The inflamed meninges get stretched when you straighten the leg.
Brudzinski sign
Passively flex the neck → patient involuntarily flexes hips and knees
Same · meningeal irritation. Flexing the neck tugs on the inflamed meninges, so the body flexes the legs to reduce the stretch.
Petechial rash
Non-blanching purple-red spots, may coalesce into purpura
N. meningitidis until proven otherwise. Endotoxin → DIC → vascular damage.
Complication of meningococcemia. Fulminant DIC destroys the adrenals. Rapidly fatal without aggressive treatment.
When to CT before LP:
Not everyone needs a CT before their LPThe fear: if there's elevated intracranial pressure from a mass lesion, doing an LP could cause brain herniation · removing CSF from below while pressure pushes the brain down. But most meningitis patients don't have focal lesions. The CT is to rule out a mass/abscess that would make the LP dangerous.. Only CT first if any of these are present:
• Immunocompromised (HIV, transplant, chemo)
• History of CNS disease (mass, stroke, focal infection)
• New-onset seizure
• Papilledema (sign of raised ICP)
• Focal neurologic deficit
• Altered consciousness
Critical: If CT is needed, give antibiotics FIRST, then CT, then LP. Never delay antibiotics waiting for a CT or LP. Every hour of delay increases mortality.
Board Trap
Don't delay antibiotics for imaging. If a patient has suspected bacterial meningitis and needs a CT before LP, start empiric antibiotics + dexamethasone IMMEDIATELY. Get blood cultures first (takes 30 seconds), then antibiotics, then CT when available, then LP. The LP can wait. The antibiotics cannot.
A 45-year-old HIV+ patient presents with fever, headache, and nuchal rigidity. You suspect meningitis. What's the correct order of operations?
Perfect. HIV = immunocompromised = CT before LP. But never delay antibiotics. Blood cultures (fast) → empiric antibiotics → CT → LP. Also think Cryptococcus in this patient · India ink stain, cryptococcal antigen.
The order matters. This patient is immunocompromised (HIV), so CT before LP is required (to rule out mass/abscess). But antibiotics come BEFORE the CT. Blood cultures → antibiotics → CT → LP. Never wait on antibiotics · every hour of delay in bacterial meningitis increases mortality by ~3-6%.
SECTION 04
Special Organisms & High-Yield Details
Organism
See It
Key Fact
N. meningitidis
Petechial rash, college dorm, military barracks
Prophylaxis for close contacts: rifampin, ciprofloxacin, or ceftriaxone. Vaccine: MenACWY + MenB.
S. pneumoniae
Elderly, alcoholic, post-splenectomy, sickle cell
#1 cause in adults overall. Quellung reactionQuellung = "swelling" in German. Mix bacteria with anti-capsular antibodies → capsule swells and becomes visible under microscopy. Classic identification test for S. pneumoniae, but PCR has largely replaced it. positive. Lancet-shaped diplococci.
Listeria
Neonates, elderly, pregnant, immunocompromised, deli meats
NOT covered by cephalosporins. Needs ampicillin. Tumbling motility at 25°C. Actin rocket tails for intracellular spread.
Cryptococcus neoformans
HIV/AIDS (CD4 <100), pigeon droppings
India ink shows encapsulated yeast. Latex agglutination for capsular antigen. Soap bubble lesions on brain MRI. Treat with amphotericin B + flucytosine.
HSV-2 (Mollaret)
Recurrent aseptic meningitis, lymphocytic CSF, normal glucose
Self-limited episodes. PCR for HSV DNA in CSF. Don't confuse with HSV-1 encephalitis (temporal lobe, hemorrhagic).
Basilar meningitis → CN palsies. CSF: lymphocytes, very high protein, very low glucose. AFB stain often negative · need PCR or culture.
Group B Strep
Neonate <7 days old, premature rupture of membranes
Screen all pregnant women at 36-37 weeks. Intrapartum penicillin prophylaxis if positive.
Adjunct Therapy
Dexamethasone · when and why:
Give dexamethasone before or with the first dose of antibiotics in suspected bacterial meningitis. It reduces inflammation and decreases mortality/hearing loss, especially in S. pneumoniae meningitis.
Do NOT give dexamethasone if:
• Already on antibiotics (too late · the inflammatory cascade already started)
• Neonatal meningitis (no proven benefit, may be harmful)
SECTION 05
Elimination Challenge
Case 1: A 3-week-old infant presents with fever, irritability, and a bulging fontanelle. CSF shows neutrophils, low glucose, and gram-positive cocci in chains. Which organism?
E. coli
Group B Strep
Listeria
N. meningitidis
Case 2: A 25-year-old HIV+ man (CD4 count 50) presents with headache and confusion over 2 weeks. CSF shows lymphocytes, elevated protein, low glucose, and elevated opening pressure. What do you see on India ink stainIndia ink stain: the particles can't penetrate the thick polysaccharide capsule, so encapsulated organisms appear as clear halos against a dark background. Classic for Cryptococcus neoformans.?
TB meningitis
Cryptococcus
HSV encephalitis
Toxoplasmosis
Case 3: A 22-year-old Marine recruit develops high fever, headache, and within hours has spreading purpura and hypotension. Blood pressure is crashing despite fluids. Labs show DIC. What devastating complication has occurred?
Cerebral herniation
Waterhouse-Friderichsen
SIADH
Subdural empyema
Decision Tree: Meningitis Empiric Treatment
Suspected meningitis. Walk through each branch. One click per step.
Signs of herniation? (focal deficits, papilledema, altered consciousness, immunocompromised)
LP done. CSF result?
Bacterial meningitis
Get blood and CSF cultures → start empiric: ceftriaxone + vancomycin + dexamethasone (give dex before or with antibiotics, not after)
Add ampicillin if immunocompromised, elderly, or infant under 3 months (Listeria coverage)
Neonates under 1 month: GBS + E. coli + Listeria → cefotaxime + ampicillin (NOT ceftriaxone: displaces bilirubin)
Viral meningitis (most likely)
Most common cause: enterovirus
If HSV cannot be ruled out (temporal lobe involvement, focal signs, CSF RBCs): treat empirically with acyclovir
Other causes: arbovirus (West Nile), mumps, HIV acute seroconversion
Most viral cases: supportive care
Subarachnoid hemorrhage, not meningitis
Xanthochromia = bilirubin from lysed RBCs in CSF → indicates bleeding, not infection
Emergent CT + neurosurgery consult. Do not treat with antibiotics for meningitis.
CT head first, then LP
Do NOT delay antibiotics waiting for CT or LP → start empiric ceftriaxone + vancomycin + dexamethasone immediately
After CT rules out herniation risk → do LP to identify organism and narrow therapy
Blood cultures before antibiotics if possible, but antibiotics cannot wait
SECTION 06
Board Quiz · Clinical Vignettes
Five third-order cases per round. Every wrong answer teaches you why. Shuffled, never-repeat.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 5, 2026 at 8:17 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.