A loose crystal rolling in a fluid loop deep in the ear, a spin that lasts seconds when you turn your head, and a single exam that tells a harmless inner ear from a brainstem stroke. Learn the mechanics, the nystagmus rules, the Dix-Hallpike, and the Epley fix.
The Setup
A Crystal in the Wrong Place
Vertigo is the false sense that you or the room is spinning. In BPPV it comes from one mechanical error deep in the ear. Walk the chain and the brief, position-triggered spin makes perfect sense.
A 56-year-old woman says that every time she rolls onto her right side in bed or tips her head back to wash her hair, the room spins violently for about thirty seconds and then settles. She has no hearing loss, no ringing, and no weakness or numbness. Between episodes she feels completely normal.
What single mechanism best explains the whole story?
Start with the sensor. The inner ear has two kinds of motion sensor. The otolith organs (the utricle and saccule) sense gravity and straight-line motion using tiny calcium carbonate crystals called otoconia that sit on a jelly pad. The semicircular canals are three fluid-filled loops that sense rotation; when your head turns, the fluid (endolymph) lags and bends a sensor called the cupulaA gelatinous flap inside each semicircular canal. When endolymph pushes against it, it bends and triggers the nerve, signaling that the head is rotating..
Now the error. In BPPV a crystal breaks loose from the utricle and tumbles into a canal, almost always the posterior semicircular canal (it sits lowest, so gravity drops crystals into it). Change head position → the heavy crystal slides through the canal → it drags the endolymph → the cupula bends → the canal screams that the head is spinning even though it has stopped. The brain gets a rotation signal the eyes do not confirm, and you feel the room whirl. This loose-crystal mechanism is called canalithiasis.
Why brief, why positional, why fatigable. The spin lasts under a minute because once the crystal finishes falling and the fluid stops moving, the false signal ends. It is positional because only certain head movements drop the crystal through the canal. And repeated testing tires it out (the crystal disperses), which is why peripheral nystagmus fatigues.
The whole disease in one line: a crystal drops into the lowest canal, head motion drags it, the false spin signal lasts only as long as the crystal is moving.
BPPV lives among other peripheral causes. All of these come from the inner ear or its nerve rather than the brain. Flip each card.
BPPVTap to flip
Loose crystals, brief spinsSeconds-long vertigo triggered by head position, no hearing loss, completely normal between spells. Confirmed by Dix-Hallpike, fixed by Epley. The most common cause of vertigo.
Vestibular neuritisTap to flip
Continuous spin, no hearing lossInflammation of the vestibular nerve, often after a viral illness. Constant severe vertigo for days, not seconds, with a positive head impulse test and preserved hearing. Add hearing loss and it becomes labyrinthitis.
Meniere diseaseTap to flip
The episodic quartetToo much endolymph (endolymphatic hydrops). Attacks of vertigo lasting minutes to hours with fluctuating hearing loss, tinnitus, and ear fullness. The hearing symptoms are what separate it from BPPV.
Clinical Images
Outer, middle, and inner ear · tap
The labyrinth: canals and otolith organs · tap
Nystagmus: the slow drift and fast jerk · tap
Epley maneuver rolls the crystal out · tap
The Big Fork
Inner Ear or Brainstem
The single most important question in any dizzy patient is whether the problem is a harmless inner ear or a dangerous brainstem. The eyes give it away. Learn the nystagmus rules and you can localize at the bedside.
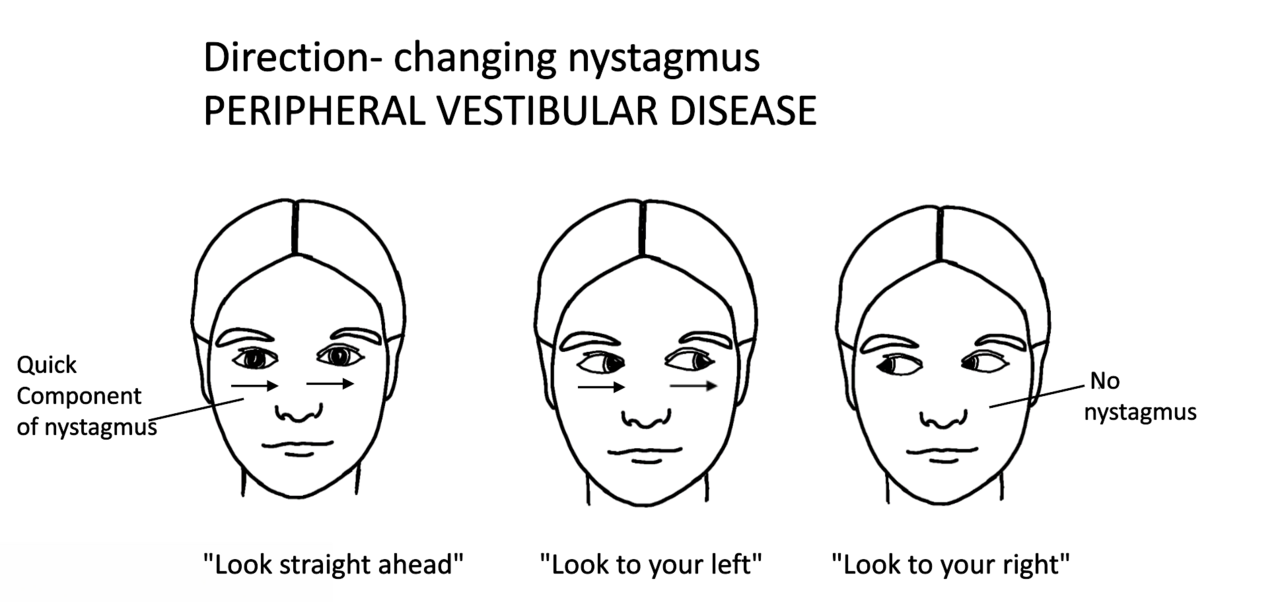
Read the eyes.Nystagmus is a rhythmic eye movement with a slow drift one way and a fast jerk back. Its pattern tells you where the lesion is. Peripheral nystagmus is horizontal or torsional, beats in one direction only, has a brief latency, fatigues with repetition, and quiets when the patient fixes on an object. Central nystagmus is the opposite: it can be purely vertical, changes direction with gaze, does not fatigue, and is not suppressed by visual fixation. Tap each feature.
Direction
Tap to reveal
Peripheral nystagmus is horizontal or horizontal-torsional and beats one way. Purely vertical or direction-changing nystagmus is central until proven otherwise.
Visual fixation
Tap to reveal
Peripheral nystagmus is suppressed when the patient stares at a fixed point. Central nystagmus keeps going despite fixation. Fixation is the brain calming a noisy inner ear, which it cannot do for a brainstem lesion.
Latency and fatigue
Tap to reveal
Peripheral BPPV nystagmus starts a few seconds after the trigger and tires out on repeat testing as the crystal disperses. Central nystagmus starts immediately and does not fatigue.
Head impulse test
Tap to reveal
Turn the head quickly while the patient fixes on your nose. An ABNORMAL test (a corrective catch-up saccade) means a peripheral lesion. A NORMAL head impulse in a patient with continuous vertigo is the scary one, pointing central.
Walking and extra signs
Tap to reveal
A peripheral patient is miserable but can walk with support. Inability to stand or walk at all, or any slurred speech, double vision, facial droop, or limb weakness, points to a central cause.
Bundle it into HINTS. The HINTS exam (Head Impulse, Nystagmus, Test of Skew) is the three-part bedside screen for a patient with continuous vertigo. The combination that points to a dangerous central cause is a normal head impulse, direction-changing nystagmus, and a vertical skew of the eyes. That trio outperforms an early MRI for catching a posterior circulation stroke.
From the Attending
The counterintuitive one trips everybody. In acute continuous vertigo, a normal head impulse test is the worrisome result, not the reassuring one. A normal response means the inner ear reflex is intact, so the problem is upstream in the brainstem. Normal head impulse plus vertical or direction-changing nystagmus equals brainstem until you prove otherwise.
Confirming It
The Maneuver That Diagnoses
For BPPV the diagnosis is a bedside maneuver, not a scan. For everything else, the history and the nystagmus sort the peripheral causes from the central ones. Work the decisions.
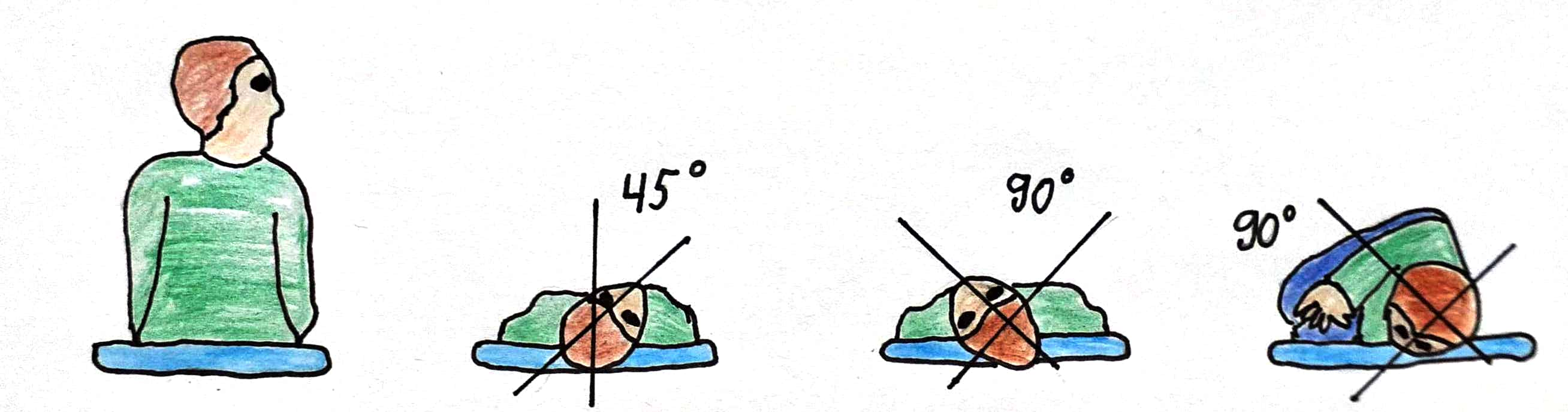
The Dix-Hallpike test. To confirm posterior canal BPPV, sit the patient up, turn the head 45 degrees toward the tested side, then lay them back quickly with the head hanging slightly off the edge. A positive test shows the BPPV signature: a brief latency of a few seconds, then upbeating, torsional nystagmus and a burst of vertigo that fatigues when you repeat it. Those features confirm a loose crystal in the canal.
A healthy 50-year-old has seconds-long spinning when she rolls in bed, normal hearing, and a normal neuro exam. Which is the best next step?
The history is textbook posterior canal BPPV, so confirm it at the bedside with Dix-Hallpike rather than scanning. A positive test shows latency, then upbeating torsional nystagmus that fatigues. Imaging is for central red flags, not for classic positional vertigo. Brief positional vertigo with normal hearing and exam? Dix-Hallpike, not MRI.
A 68-year-old with hypertension has continuous vertigo. On HINTS his head impulse is normal, his nystagmus changes direction with gaze, and there is a vertical skew. What does this combination indicate?
This is the dangerous HINTS pattern. A normal head impulse means the inner ear reflex is intact, so the lesion is central. Add direction-changing nystagmus and a skew and you have a brainstem or cerebellar stroke until proven otherwise. Get MRI and admit. Normal head impulse plus direction-changing nystagmus plus skew equals central.
A 30-year-old has three days of constant severe vertigo after a cold. His hearing is normal, his head impulse test is positive on one side, and there are no other neuro signs. Which is the most likely diagnosis?
Continuous vertigo for days after a viral illness, a positive head impulse, and preserved hearing is vestibular neuritis (the vestibular nerve is inflamed). BPPV is seconds long and positional, and Meniere brings hearing loss, tinnitus, and fullness. Add hearing loss to this picture and it becomes labyrinthitis. Days of constant spin, normal hearing, positive head impulse equals vestibular neuritis.
Sort the whole field. The table lines up the peripheral causes against the central one so the discriminators stay clear.
Cause
Timing and clues that point to it
BPPV
Seconds of vertigo, triggered by head position, no hearing loss. Positive Dix-Hallpike. Treated with Epley.
Vestibular neuritis
Days of continuous vertigo after a viral illness, normal hearing, positive head impulse, no other neuro signs.
Labyrinthitis
Like vestibular neuritis but WITH hearing loss, because the cochlea is involved too.
Meniere disease
Attacks of minutes to hours with fluctuating hearing loss, tinnitus, and ear fullness. Endolymphatic hydrops.
Posterior stroke
Continuous vertigo with central nystagmus, normal head impulse, skew, or inability to walk. Risk factors and other brainstem signs.
Vestibular migraine
Recurrent vertigo with headache, light sensitivity, and a migraine history. No hearing loss between attacks.
Board Trap
Do not let an early normal CT or MRI talk you out of a stroke. A plain CT misses most early posterior fossa strokes, and even MRI can be falsely normal in the first day or two for a small infarct. In acute continuous vertigo, a careful HINTS exam beats early imaging for catching a brainstem stroke. The exam outranks the early scan here.
The Plan
Roll the Crystal Home
BPPV has an elegant mechanical cure that needs no drugs. The other peripheral causes get short symptom relief and rehab. The tested mistake is reaching for long-term suppressants.
BPPV: the Epley maneuver. Since the problem is a crystal in the wrong loop, the fix is to roll it back out. The Epley canalith repositioning maneuver is a sequence of head turns that walks the crystal through the canal and back into the utricle, where it no longer triggers the canal. It cures most patients in one or a few sessions, no medication required.
Skip the long-term pills. Vestibular suppressants like meclizine or a short benzodiazepine can blunt a severe acute spin for a day or two, but using them for weeks is a mistake: they stop the brain from re-learning balance (central compensation) and leave the patient dizzy longer. For BPPV specifically, the maneuver is the treatment, not the drug.
The other peripheral causes.Vestibular neuritis gets a few days of symptom relief plus early vestibular rehabilitation, and steroids may shorten the course. Meniere disease is managed with a low-salt diet, a diuretic, and trigger avoidance to reduce the fluid pressure, with procedures reserved for refractory cases. Vestibular migraine is treated like migraine.
From the Attending
When a young, otherwise healthy patient has classic positional vertigo and a positive Dix-Hallpike, the right answer is to perform the Epley and send them home, not to admit and scan. Save the imaging and the admission for the central red flags. Match the workup to the localization, and most dizzy patients never need a scanner.
Board Trap
A stem that hands you a textbook BPPV patient and then offers daily meclizine for a month is testing whether you know the cure is mechanical. Choose the Epley maneuver. Long-term suppressants are the wrong answer dressed up as treatment. The crystal needs to move, not the patient sedated.
Prove It
Board Walkthrough
Seven original clinical vignettes, 5 dealt per round, answer choices shuffled, never repeating within a round. Tap a wrong answer first to see why it almost works, then read the glowing clues.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.