Na+/K+ pump goes down. Water floods in. Cell BLOATS. Every injury, every disease, same first move.
Na+/K+ PumpHydropic ChangeHeart vs Brain6 Necrosis Patterns
Opening Case
Here is your patient: A 58-year-old man has a massive heart attack. Blood flow to his cardiomyocytes stops cold. His pathologist is called to the scene. Which is the very first microscopic change she will see if she looks at those cells 30 minutes later?
Nuclear pyknosis (shrinkage)
Cellular swelling (hydropic change)
Ghost cell outlines forming
Membrane rupture with enzyme release
Nuclear pyknosis, ghost cells, and membrane rupture are all signs of irreversible injury. They come much later. The very first thing that happens is embarrassingly simple. You know how when a pump at a pool breaks, the water level rises? That is literally what happens here. The Na+/K+ pump needs ATP to run. No blood flow means no oxygen means no ATP. Pump stops. Sodium piles up inside. Water follows sodium (osmosis is a law, not a suggestion). The cell bloats. That is it. That is the first sign. Cellular swelling = hydropic change = THE first sign of any reversible injury. Every time.
From the Attending
Cellular injury clinical questions trace one chain: insult -> ATP depletion -> Na+/K+ pump fails -> sodium pulls water in -> cell swells (reversible). If oxygen comes back here, the cell lives. Cross the line and you get membrane breakdown, Ca²⁺ flood, mitochondrial permeability transition pore opening -> that's it, irreversible.Every stem you'll see is asking which side of that line the patient is on. The clue is almost always the histology: cell swelling = reversible; membrane disruption + nuclear changes (pyknosis/karyorrhexis/karyolysis) = past the point of no return.
Reversibility Stopwatch
Drag the slider. Watch the cell change shape and the verdict flip. The 30-minute line is the point of no return for warm ischemia.
Ischemia Timer
A myocyte deprived of O2. ATP falls, the Na+/K+ pump stalls, water creeps in, then calcium overruns it. Slide right and watch the cell go from swollen-but-saveable to mitochondrial-permeability-pore catastrophe.
0 min
warm ischemia time
point of no return · 30 min
REVERSIBLE
ATP drops > 50% · Na+/K+-ATPase stalls
Cellular swelling, ribosome detachment
Fatty change (reversible, develops over hours)
ER swelling, mitochondrial swelling
Irreversible · past the 30 min line
Ca²⁺ influx (irreversible threshold)
Mitochondrial permeability transition pore opens
Membrane phospholipid breakdown
Nuclear pyknosis (shrunken) · histology, hours later
Karyorrhexis / karyolysis (dissolved) · histology, 1 to 3 days later
From the Attending
Reversible vs irreversible cellular injury hinges on three anchors: Ca²⁺ influx, mitochondrial permeability transition pore opening, and membrane phospholipid breakdown. Cross any of those and the cell is dead. The 30-minute line for warm ischemia is the clinical medicine anchor · before 30, reperfusion saves the cell; after 30, reperfusion just lets calcium in faster. Nuclear changes (pyknosis -> karyorrhexis -> karyolysis) are the histology proof you missed the window, and they appear hours to days later (pyknosis about 12 to 24 h, karyolysis 1 to 3 days), not in the first hour.
The Pump Cascade
One reversible chain: ATP falls, the Na+/K+ pump stalls, sodium stays in, water follows, and the cell swells.
Path · Cell Injury
Pump online
Pump workingATP drives 3 Na+ out, 2 K+ in.
ATP goneThe pump loses power.
Na+ trappedSodium can no longer leave.
Water entersCell swelling begins.
OUTSIDE CELLNa+ normally lives out hereNa+Na+K+K+H2OH2O
Pump
INSIDE CELL
ATP source
ATPNa+Na+Na+K+K+H2OH2O
ATP powers the Na+/K+ pump: 3 Na+ out, 2 K+ in. Sodium stays low inside, so water stays put.
Pattern Anchored · Cell 47
The Reversible Injury Chain
RouteIschemia -> O2 down -> ATP down -> Na+/K+ pump stalls -> Na+ held inside -> H2O follows -> cell swells
PatternHydropic change: pale/cloudy cytoplasm, swollen ER, ribosomes falling off rough ER. Ugly, but still reversible.
PearlSwelling is the warning light, not the funeral. Restore ATP before Ca2+ floods in and the pump can recover.
🎯What will you do next time? cell swelling/hydropic change is the earliest visible sign of reversible cell injury. It happens before nuclear changes, membrane rupture, or enzyme leak.
⚠Board trap: fatty change (steatosis) is also reversible but NOT the first sign. Swelling comes before fat accumulates.
From the Attending
The Na+/K+-ATPase is the canary. It eats 30·60% of cellular ATP just to push 3 Na out and 2 K in. Drop ATP, the pump stalls. Sodium accumulates intracellularly · chloride and water follow · the cell swells. This is the FIRST morphologic change you can see on H&E. Stem says "hydropic change" or "cellular swelling on biopsy after a hypoxic event"? That's a stalled pump. Stem says "post-mortem on a patient who arrested 3 minutes ago and got prompt ROSC, cell architecture preserved"? Reversible. Memorize the pump dependency · everything else is downstream.
The Point of No Return
Calcium is kept outside the cytosol. When the membrane fails, Ca2+ floods in and turns quiet housekeeping enzymes into demolition enzymes.
Path · Point of No Return
Calcium outside
Cytosolic calcium is kept low. Membranes and Ca2+ pumps hold a huge gradient outside the cytosol.
Pattern Anchored · Calcium
The Irreversible Injury Switch
RouteMembrane injury + pump failure -> Ca2+ floods in -> PLA2, proteases, endonucleases, and ATPases turn on.
PatternPLA2 chews membranes. Proteases cut cytoskeleton. Endonucleases fragment DNA. Those three are the structural executioners above; calcium also drives ATPases to burn the last ATP as the mitochondrial pore opens.
PearlNa+ water swelling can reverse. Ca2+ enzyme activation means the cell has crossed the line.
⚠Board trap: calcium also opens the mitochondrial permeability transition pore. Flocculent mitochondrial densities = irreversible injury on histology.
Decision Tree
Three calls. The right answer teaches the mechanism. The wrong one teaches the trap.
1
A hepatocyte has been without oxygen for 20 minutes. You look under the microscope and see:
swollen cell, ER dilation, ribosomes detaching from rough ER, no membrane rupture.
What is the injury status?
Reversible injury. The cell can still be saved.
Irreversible injury. This cell is already dead.
2
Blood flow is restored at the 20-minute mark. Which finding tells you this cell will survive?
The Na+/K+ pump restores and the cell shrinks back to normal size.
Calcium floods into the cytoplasm from the ER and extracellular space.
3
New scenario: 4 hours of ischemia. Gross pathology shows a pale infarct in the wall of the left ventricle. Histology: ghost-like cell outlines with preserved architecture, no nuclei visible. What type of necrosis?
Coagulative necrosis. The myocardium is the classic example.
Liquefactive necrosis. The heart liquefied because it ran out of blood.
Caseous necrosis. The heart tissue looks cheesy under the microscope.
Board Trap: Apoptosis vs Necrosis
Feature
Apoptosis
Necrosis
Energy required
Yes (ATP needed)
No (passive, catastrophic)
Cell count
Individual cells
Groups of cells
Inflammation
None
Yes (membrane rupture triggers it)
Membrane
Intact until phagocytosis
Ruptures
Fate
Apoptotic bodies (phagocytosed)
Debris, inflammatory response
Executor
CaspasesCysteine proteases that cleave after aspartate residues. "Casp" = cysteine aspartate protease. Activated by intrinsic (mitochondrial) or extrinsic (death receptor) pathway.
Three irreversibility markers: (1) Ca²⁺ flood (cell can't keep it out), (2) MPTP opens (cytochrome c leaks, ATP production permanently dead), (3) Membrane phospholipid breakdown by Ca-activated phospholipases. The histology giveaway is nuclear: pyknosis (shrunken dark), karyorrhexis (fragmented), karyolysis (dissolved). Any of those three nuclear changes = the cell is dead. clinical medicine love the calcium step · it's the gate.
Heart vs Brain
Ischemia usually leaves ghost architecture. The brain breaks the rule and melts into a cavity.
Heart Infarct
Coagulative
Alive myocardium
Dead, but outlines remain
Architecture intact
Ghost cells = coagulative
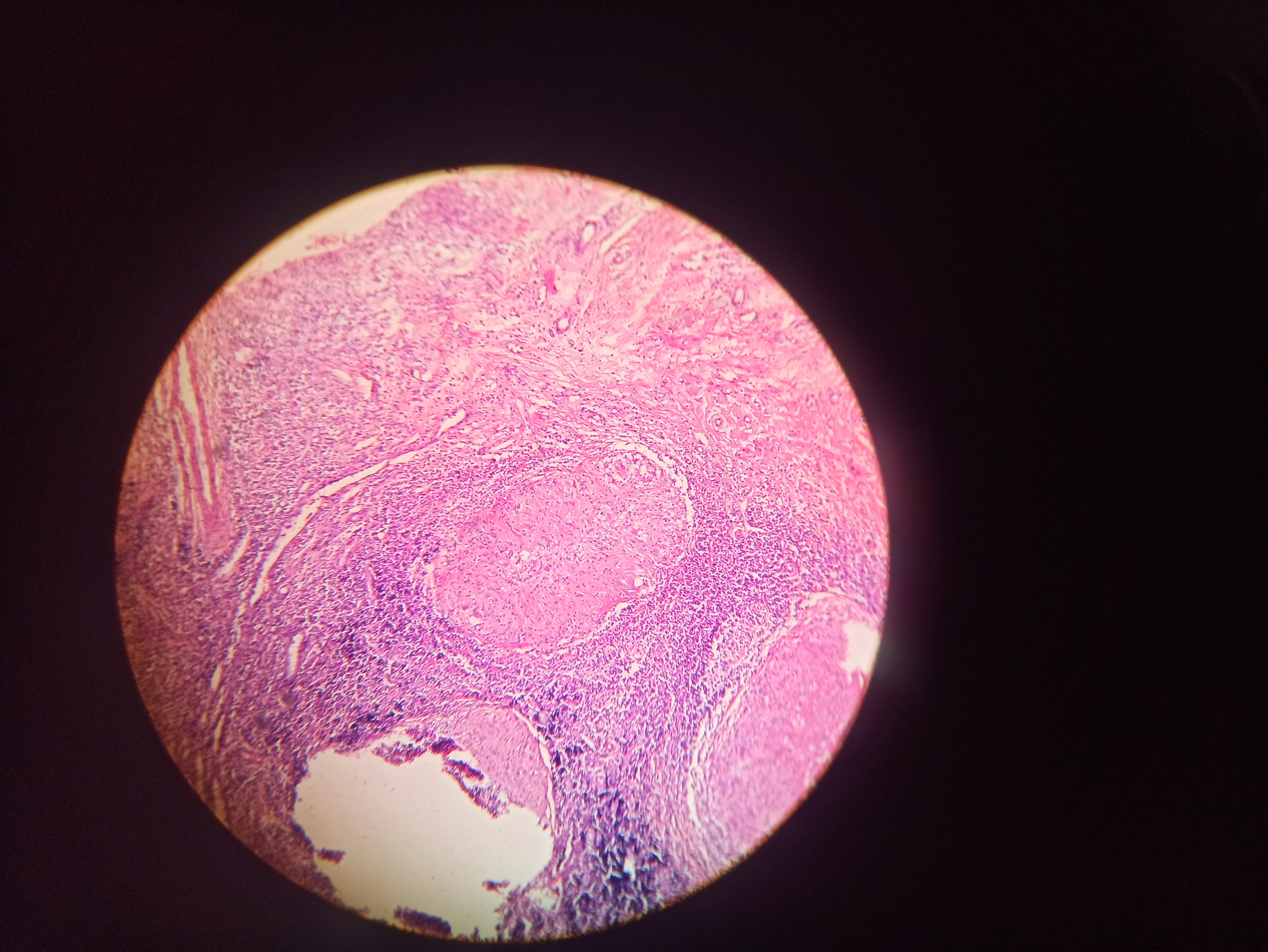
In solid organs, ischemia denatures proteins before enzymes can liquefy the tissue. Myocardial fibers become ghost outlines: nuclei vanish, architecture remains.
📷 Coag necrosis · cardiomyocyte ghosts
Brain Infarct
Liquefactive
Alive brain tissue
Architecture lost
No infarct cavity yet
Fluid cavity = liquefactive
Brain has little collagen architecture to preserve the ruins. Lysosomal enzymes and microglia digest dead tissue into a fluid cavity. Pyogenic abscesses liquefy by neutrophil enzymes.
📷 Liquefactive · cerebral cavity
Board Trap · The Brain Rule
Every solid organ infarct is coagulative except the brain. Why? Brain tissue is lipid-rich with little collagen/stromal architecture, so enzymes digest the dead tissue instead of leaving a preserved outline. The other classic mimic is a pyogenic abscess, where bacteria recruit neutrophils whose enzymes liquefy the tissue.
Preserved architecture->Coagulative
Liquefied cavity->Brain or abscess
The Necrosis Atlas
Four more patterns. Tap any card to reveal mechanism and the next move.
📷 CASEOUS NECROSIS · TB
Caseous
TB · Fungi (histoplasma, coccidioides)
HallmarkCheese-like central necrosis surrounded by granuloma
ArchitectureNOT preserved (unlike coagulative)
EtiologyTB until proven otherwise in clinical practice
🧀 Central necrosis + granuloma rim = TB
tap to flip ->
The Cheese Analogy
What You See
Grossly it looks like soft white cheese. Histologically it is amorphous pink debris with NO preserved outlines (ghost cells). Surrounded by a rim of epithelioid macrophages and giant cells (the granuloma). You know how old cheese crumbles? That is what caseous necrosis feels like to cut.
Anchor It
Any question with granuloma + central necrosis + lung/lymph node = TB first, fungal second. The granuloma is the immune system trying to wall off the infection. Caseous = TB until proven otherwise. Period.
📷 FAT NECROSIS · pancreatitis
Fat Necrosis
Pancreas (enzymatic) · Breast (traumatic)
EnzymaticLipase digests fat -> saponification
Key signChalky white deposits (Ca soap)
TraumaticBreast trauma -> oil cysts
💊 Chalky white spots + pancreatitis = fat necrosis
tap to flip ->
Saponification = Soap Formation
Trace It
In pancreatitis, lipase escapes from damaged acinar cells and digests the fat cells in the omentum. Free fatty acids are released. These bind calcium to form calcium soaps. That is literally saponificationSapon = Latin for soap. The same chemistry used to make soap: fatty acid + alkali (here, Ca2+) = soap. This is why you see chalky white deposits at autopsy.. The chalky white spots in a pancreatitis patient are these calcium-fatty acid complexes.
Anchor It
Patient with pancreatitis + chalky white peritoneal nodules at laparotomy = fat necrosis with saponification. Serum calcium may be LOW because it gets trapped in the fat. Watch for hypocalcemia in pancreatitis for this reason.
📷 FIBRINOID NECROSIS · vessel wall
Fibrinoid
Autoimmune · Immune complex disease
LocationBlood vessel walls
LookPink, amorphous, fibrin-like deposits
DiseasesSLE, PAN, malignant HTN, rheumatic fever
🔴 Pink vessel walls = fibrinoid necrosis
tap to flip ->
The Vessel Wall Problem
Trace It
Immune complexes or high pressure damage the vessel wall. Plasma proteins including fibrin leak into the wall and the wall undergoes a special necrosis that looks bright pink and homogeneous under H&E. It is called fibrinoid because it looks like fibrin, even though it is a mix of proteins. The key: it is always in vessel walls.
Anchor It
Any question about vasculitis (PAN, SLE, ANCA) that shows vessel wall pathology = think fibrinoid. Malignant hypertension classically shows fibrinoid necrosis of arterioles. Bright pink smudgy vessel wall = fibrinoid. Always.
📷 GAS GANGRENE · Clostridium
Gangrenous
Limbs · GI tract
DryCoagulative only. Ischemia without infection.
WetCoagulative + liquefactive. Infection added.
GasClostridium perfringens. Crepitus on exam.
🐛 Crepitus + gas on x-ray = gas gangrene = Clostridium
tap to flip ->
Wet vs Dry vs Gas
Dry Gangrene
Pure ischemia of a limb. No infection. Tissue mummifies (dries out, turns black). This is just coagulative necrosis of a whole limb. Think: diabetic with poor circulation in the foot, toe turns black and dry.
Wet Gangrene
Ischemia PLUS infection. The infection adds liquefactive necrosis on top of the coagulative. The tissue becomes swollen, moist, malodorous. More dangerous because infection spreads.
Anchor It
Crepitus = gas gangrene = emergency surgery + PCN G.
Board Walkthrough
One clinical vignette at a time. Shuffle the bank, mark choices, then reveal the reasoning.
From the Attending
Cellular injury vignette playbook: (1) Identify the insult (hypoxia, ischemia, free radical, toxin, infection, immune, genetic, nutritional). (2) Locate the cell on the timeline · reversible (swelling, fatty change, ribosome detachment) or irreversible (Ca flood, MPTP open, membrane rupture, pyknosis/karyorrhexis/karyolysis). (3) Name the necrosis pattern if dead · coagulative (heart, kidney, infarct), liquefactive (brain, abscess), caseous (TB), fat (pancreas, breast), fibrinoid (vessels), gangrenous (limb). The pattern names the organ. The organ names the pattern. Anchor that pairing first · it's how every stem closes.
Medically reviewed by Fatima Ali, DO and Kaitlyn Cocuzzo, MD · Last updated July 2, 2026 at 4:04 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.