The testable pattern is not just "nephrotoxic." Foscarnet is a pyrophosphate analog that skips viral kinase activation, hits viral polymerase directly, and then punishes the patient with kidney injury plus divalent-ion chelation.
From the Attending
If the stem says ganciclovir or acyclovir stopped working, ask one question first: did the virus break the activation step? Foscarnet matters because it does not need that step. Then immediately ask what the drug is doing to calcium, magnesium, phosphate, potassium, and creatinine.
Opening challenge
A 36-year-old man with AIDS has CMV retinitis that progresses despite therapeutic ganciclovir levels. Genotyping shows a viral kinase mutation that prevents drug activation. The team switches to foscarnet. What toxicity should be watched most closely in the first week?
Right. Foscarnet bypasses kinase activation, but it chelates divalent ions and injures renal tubules. Watch ionized calcium, magnesium, phosphate, potassium, and creatinine together.
Mechanism theater
The phosphate decoy jams the viral machine
Press the stages. The animation shows why foscarnet does not care about thymidine kinase or CMV kinase resistance, then why the same phosphate chemistry drags calcium and magnesium into the toxicity story.
Growing DNA strand
Divalent ions Ca / Mg
Pyrophosphate pocket
No kinase needed
Ionized Ca 1.30 mmol/L Magnesium 2.0 mg/dL
Tap a stage
No kinase needed
Acyclovir and ganciclovir are prodrugs: a viral kinase has to switch them on. If that kinase is mutated, they stall at a dead gate. Foscarnet arrives already active and walks straight to the polymerase.
RouteSkips viral kinase activation
PatternBeats TK-deficient HSV and UL97-mutant CMV
PearlNo kinase step means kinase resistance cannot lock it out
Toxicity triage
Do not memorize one electrolyte
Foscarnet is a cluster problem: calcium, magnesium, phosphate, potassium, and creatinine all move together. The board trick is deciding which abnormality is driving the symptom in front of you.
Ionized calcium
Tetany, QT prolongation, seizures
Foscarnet can lower ionized calcium through divalent-ion chelation. Total calcium may not tell the whole story. If the patient has perioral tingling, carpopedal spasm, or seizures, think ionized calcium first.
Magnesium
The correction blocker
Low magnesium lowers seizure threshold and makes potassium and calcium harder to correct. If potassium refuses to rise, replete magnesium instead of just pushing more potassium.
Kidney
The amplifier
Renal tubular injury raises foscarnet exposure and destabilizes the electrolyte panel. Hydration and renal adjustment are not boring details. They are the thing preventing the toxicity cascade.
From the Attending
Do not answer "hypocalcemia" reflexively. Ask what the stem is showing. Tetany or seizure with low ionized calcium points to calcium. Refractory hypokalemia points to magnesium. Rising creatinine points to the kidney as the reason the whole panel is getting worse.
Patient on foscarnet develops perioral tingling and carpopedal spasm. What panel do you check first?
Ionized calcium is the active fraction. Foscarnet chelation can make that fraction dangerous even when the total calcium looks less dramatic.
Next step unlocked: after calcium, ask whether magnesium is preventing correction.
The potassium is low and will not correct despite replacement. What hidden problem should you fix?
Low magnesium keeps renal potassium wasting alive. Replete magnesium or the potassium bag is just expensive decoration.
Next step unlocked: look at creatinine so you do not keep dosing into kidney injury.
Creatinine rises during therapy. What action prevents the toxicity spiral from worsening?
Hydration and renal adjustment are the foscarnet kidney move. Probenecid belongs to cidofovir, and oral foscarnet is not the clinical route.
Pattern locked: foscarnet rescue requires kidney and electrolyte surveillance from the start.
Clinical routing
When to reach for it
Foscarnet is not a gentle default. It is the direct polymerase tool when kinase-activated antivirals fail or when marrow toxicity makes ganciclovir dangerous.
Ganciclovir: great for CMV until the activation step breaks
Needs viral CMV kinase activation, then host kinases finish the job. Main toxicity is marrow suppression. If the ANC is already low, this drug can turn a viral problem into a neutropenic bacterial problem.
Foscarnet: no kinase gate, direct polymerase block
Does not require phosphorylation. That is the rescue logic for kinase-resistant HSV or CMV activation failure. The tradeoff is kidney and electrolyte surveillance.
Cidofovir: another polymerase option, different protection rule
Uses host phosphorylation and is strongly nephrotoxic. The protectant association is probenecid plus hydration. Do not import that probenecid rule into foscarnet questions.
FOS = phosphate feel
It mimics pyrophosphate, so it slots into the polymerase exit pocket and blocks the next base.
Tap to reveal
No kinase, no permission slip
Foscarnet walks past the activation checkpoint already active, so TK-deficient HSV and UL97-mutant CMV cannot lock it out.
Tap to reveal
Two monitors travel together
Creatinine tells you exposure risk; ionized calcium and magnesium tell you seizure and rhythm risk.
Tap to reveal
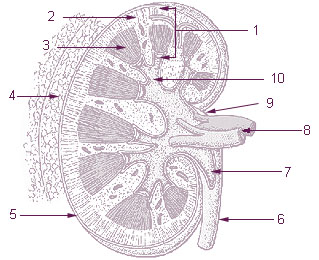
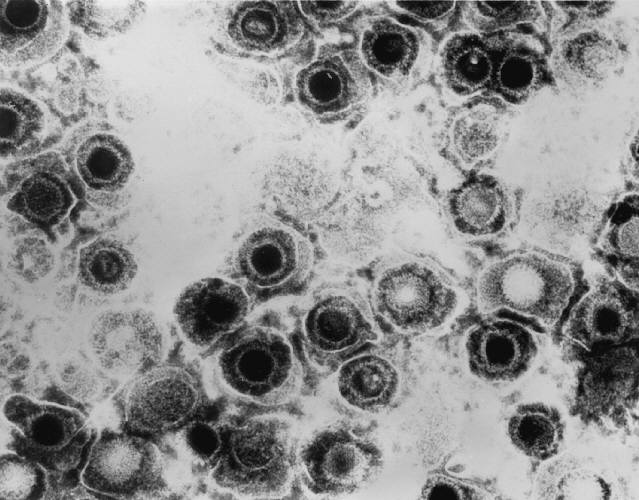
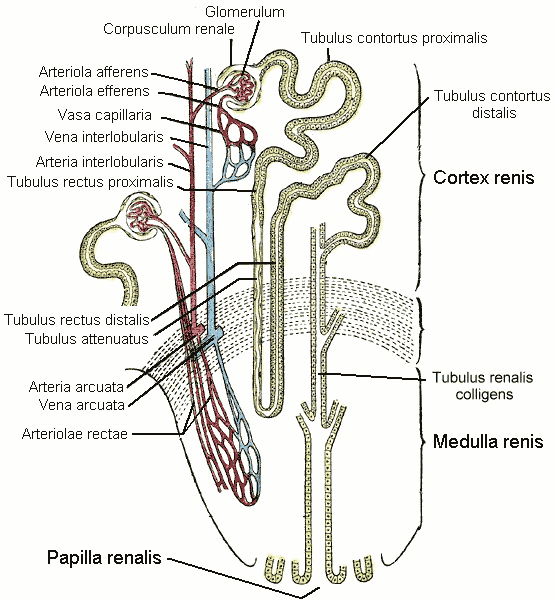
Image strip
Tap any image to expand. The photos anchor the actual disease targets and the kidney/electrolyte context without putting fake labels on real images.
Use the exam tools before you answer: right-click or long-press to cross out, double-click or double-tap to highlight. The highlighted clues glow only after you commit.
Medically reviewed by Fatima Ali, DO and Kaitlyn Cocuzzo, MD · Last updated July 2, 2026 at 4:04 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.