A patient on long-term prednisone shows up with three problems that look unrelated. They are not. Follow the cluster.
A 54-year-old woman with rheumatoid arthritis is referred to endocrinology. She reports weight gain, easy bruising, and new-onset hyperglycemia (fasting glucose 148 mg/dL, normal 70-99). On physical examination she has central adiposity, a dorsal fat pad, and moon facies. Blood pressure is 152/96 mmHg. DEXA reveals hip T-score of -1.9 and lumbar spine T-score of -2.1. Which single agent most likely produced all of these findings?
The cluster is the clue: hyperglycemia plus fat redistribution plus osteopenia plus hypertension is the Cushingoid fingerprint. Prednisone does all four through overlapping mechanisms: gluconeogenesis drives glucose up, cortisol redistributes fat centrally, osteoblast suppression drains bone, and mineralocorticoid activity retains sodium and raises blood pressure. Every time you see osteopenia alongside metabolic and fat clues, land on chronic glucocorticoids first.
From the Attending
The stem gives you four findings and asks for one drug. The clinical medicine reward the student who reads the cluster, not the one who chases individual symptoms. Osteopenia alone has a long differential. Osteopenia plus Cushingoid features has one answer: chronic glucocorticoids. Know your clues.
How Steroids Drain Bone
Three exits. One source. One outcome. Watch the mechanism unfold.
Build side: glucocorticoids switch off osteoblasts -> new bone stops being made.
Break side: OPG goes down -> osteoclasts lose their brake -> resorption accelerates.
Calcium side: 1-alpha-hydroxylase blocked -> active vitamin D falls -> gut absorbs less, kidney wastes more.
Bone Budget Simulator
Shift exposure level and watch the balance tilt.
Osteoblast Output
Osteoclast Pressure
Net DEXA Trend
From the Attending
Three mechanisms hit simultaneously. Build stops. Breakdown rises. Calcium absorption drops. You do not need to memorize doses to answer these questions; you need to know that every one of these goes the wrong direction at the same time. That is why steroid bone loss accelerates fast and stays hard to reverse even after stopping the drug.
Bone Pathology: What It Looks Like
Tap any image to enlarge. Each anchors a testable clinical concept.
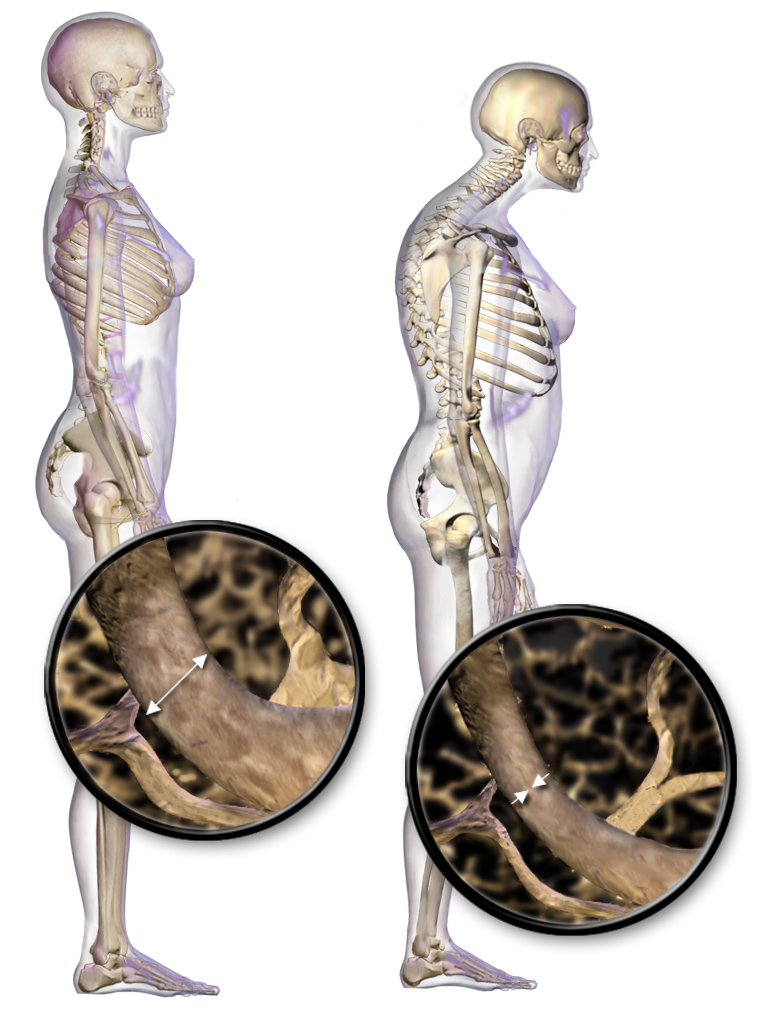
Trabecular thinning. Steroid osteoblast suppression reduces density and connectivity of the inner spongy matrix.Vertebral compression fracture. Steroid osteoporosis hits trabecular-rich vertebral bodies first, causing height loss and kyphosis.DEXA lumbar spine. T-score vs. peak young-adult bone mass. Below -1.0 is osteopenia; below -2.5 is osteoporosis.
Pattern Challenge
Match the profile to the drug class before the full walkthrough.
Node 1: A patient on a biologic for RA develops reactivation of latent tuberculosis with no Cushingoid features. Which drug class is responsible?
Node 2: A patient develops dyspepsia, a gastric ulcer, and elevated creatinine after starting an anti-inflammatory drug for gout. No fat redistribution or hyperglycemia. Which class?
Node 3: A patient on long-term therapy for SLE develops central adiposity, hyperglycemia, and DEXA T-score -2.0. Which drug class?
The pattern grid: TNF inhibitors -> infections (TB reactivation). NSAIDs -> GI and renal injury. Glucocorticoids -> the metabolic-bone-fat triad. Hydroxychloroquine -> retinal toxicity (bull's eye maculopathy). One cluster, one drug class.
Board Walkthrough
Original clinical vignettes one at a time. Cross out choices. Highlight your pick. Never-repeat tracking resets when the pool is exhausted.
Question 1 of 5
Memory Hooks
Tap each to expand.
From the Attending
Three rules you need cold: (1) Every patient starting chronic steroids gets calcium 1200 mg plus vitamin D 1000 IU, day one, no exceptions. (2) T-score below -1.5 or any fragility fracture on steroids means add bisphosphonate. (3) Hip pain plus high-dose steroids plus MRI crescent sign means think osteonecrosis, not fragility fracture. Bisphosphonates do not prevent osteonecrosis. Know the difference. Every time.
Medically reviewed by Fatima Ali, DO and Kaitlyn Cocuzzo, MD · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.