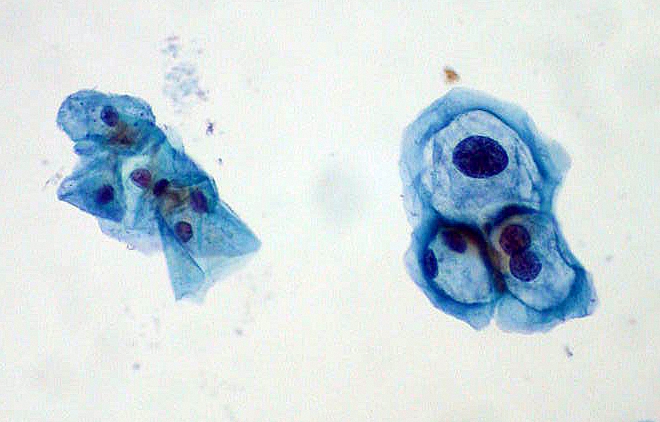
Koilocytes · raisinoid nuclei + perinuclear halo · tap to expand
CIN · dysplastic epithelium at transformation zone · tap to expand
HPV · E6/E7 oncogenes drive dysplasia · tap to expand
🔬
Cervical Cancer Screening, HPV and Dysplasia
HPV infects the transformation zone → breaks tumor suppressors → dysplasia climbs the ladder → screening catches it before invasion.
A 24-year-old woman presents for routine gynecologic care. She is sexually active with one male partner, uses condoms inconsistently, and has no symptoms. Her last Pap smear at age 21 was normal. Today, repeat cytology returns ASC-US (atypical squamous cells of undetermined significance). She asks whether she has cancer and what happens next.
What is the most appropriate next step in management?
Immediate colposcopy with biopsy
LEEP excision of the cervix
Reflex high-risk HPV testing
Repeat Pap smear in 12 months without further testing
The Cause Chain
HPV → Dysplasia → Cancer
Tap each card. Front = the step. Back = the mechanism clinical medicine test.
HPV
Basal infection
tap
Entry point
High-risk HPV (types 16 and 18 cause most cancers) infects basal cells at the squamocolumnar junction. Microtrauma from sex gives the virus access.
E6
p53 destroyed
tap
Oncoprotein 1
Viral E6 tags p53 for degradation. No p53 = no apoptosis when DNA is damaged. Damaged cells keep dividing instead of dying.
E7
Rb inactivated
tap
Oncoprotein 2
Viral E7 binds Rb, releasing E2F. The cell cycle lock is picked. Uncontrolled proliferation begins.
CIN
Dysplasia ladder
tap
Histology grades
CIN 1 = LSIL (mild, often regresses). CIN 2/3 = HSIL (moderate/severe, treat). Invasive cancer breaches the basement membrane.
Koilocyte
Cytopathic effect
tap
Pap clue
Perinuclear halo + wrinkled ("raisinoid") nucleus = koilocyte. Pathognomonic for active HPV cytopathic effect on cytology.
Why the transformation zone is the bullseye
Squamocolumnar junction: columnar epithelium meets squamous epithelium. As estrogen shifts with age/pregnancy, columnar epithelium is replaced by squamous metaplasia, creating the transformation zone.
Metaplastic cells are vulnerable: rapidly dividing basal-like cells are the perfect HPV target. Most dysplasia and cancer start here.
Years, not weeks: persistent high-risk HPV → CIN → invasion typically takes 10 to 15 years. That window is why screening works.
Clearance vs persistence: most HPV infections clear in 1 to 2 years (especially under 30). Persistence drives dysplasia. HPV-positive at 30+ is higher risk.
💡Board lock: HPV 16/18 + E6 (p53) + E7 (Rb) = the molecular chain. Koilocytes = HPV on Pap. Transformation zone = where cancer starts.🔑E6 kills the brake (p53). E7 releases the gas (Rb/E2F). Koilocyte = raisin nucleus + halo.
Who and When
Screening Guidelines
USPSTF/ACOG intervals the clinical medicine love. Age is the first fork.
Presentation (when symptomatic)
Early invasive disease is often asymptomatic. When symptoms appear, clinical medicine reach for:
Abnormal vaginal bleeding: intermenstrual or postmenopausal bleeding in older patients.
Watery/bloody discharge: advanced disease with necrosis.
Pelvic pain: late finding (parametrial invasion, obstruction).
Age < 21
No routine screening, even if sexually active.
Why: HPV is extremely common in teens and usually clears. Screening this young leads to overtreatment of transient dysplasia.
Ages 21 to 29
Pap smear every 3 years. No routine HPV co-testing.
Why: cytology catches significant lesions; HPV testing in this age group is too sensitive (most infections are transient).
Ages 30 to 65
Choose one: Pap q3y, OR HPV alone q5y, OR co-test (Pap + HPV) q5y.
Why: after 30, persistent HPV is more meaningful. HPV-first or co-test extends safe intervals.
Age > 65
Stop screening if adequate prior negative screens and not high risk.
Why: low new cancer incidence if prior screening was sufficient. Continue if history of CIN2+ or inadequate prior screening.
⚠
ASC-US triage trap
ASC-US is the most common abnormal Pap. In women ≥ 25 (and per current ASCCP pathways for 21 to 24 as well in many algorithms), reflex high-risk HPV testing is the next step. HPV negative → repeat Pap in 3 years. HPV positive → colposcopy. Do not jump to LEEP for ASC-US.
Interactive Triage
Cervical Screening Decision Tree
Pick the patient age bracket. Each branch reveals the guideline interval and the one rule that locks it in.
The patient asks about cervical cancer screening. What is her age?
No screening. Age under 21 is a hard floor regardless of sexual activity, HPV exposure, or number of partners. HPV is near-universal in adolescents and almost always clears within 1 to 2 years on its own. Screening under 21 detects transient infections, generates unnecessary colposcopies, and exposes a young cervix to LEEP, which raises the risk of preterm birth later.
Interval: none. Come back at 21.
Pap smear (cytology) every 3 years. HPV co-testing is not recommended under 30. In this age window most HPV infections still clear spontaneously, so adding HPV testing generates too many positive results that would drive overtreatment. Cytology alone catches the significant dysplasia that does not regress.
Rule: cytology q3y from 21 to 29. No HPV primary screening under 30.
Three guideline-acceptable options. Pick the modality:
Which testing strategy?
Preferred (USPSTF 2018). High-risk HPV testing alone every 5 years. A negative HPV test at 30+ gives strong reassurance because persistent high-risk HPV is the necessary precursor for all dysplasia. No HPV = very low cancer risk over the next 5 years.
Acceptable. Co-testing (Pap plus high-risk HPV) every 5 years. Both tests run on the same sample. A double negative extends the safe interval to 5 years. Historically the dominant guideline choice; now co-equal with HPV primary testing.
Acceptable. Pap smear alone every 3 years. Shorter interval than HPV-based strategies because cytology alone is less sensitive for glandular lesions and some missed HSIL. Still guideline-compliant when the patient or provider prefers cytology.
Stop screening if adequate prior screening history: 3 consecutive normal cytology results OR 2 consecutive negative co-tests in the past 10 years, most recent within 5 years. Continue screening if prior CIN 2+ or inadequate prior history.
Rule: after adequate history, new cervical cancer is rare enough that continued screening causes more harm (biopsies, anxiety, procedures) than it prevents. Inadequate prior screening means keep going.
A parent asks when to start the HPV vaccine series for a healthy child. Which window is the routine schedule?
Age 9 is the minimum approved age for the vaccine series (0 and 6 to 12 months dosing). It can be started at 9, but 9 is the floor, not the routine target. The routine recommendation is 11 to 12.
Correct. ACIP routine schedule: age 11 to 12, with the series able to start at 9. The goal is pre-exposure immunization years before typical sexual debut, when the immune response is also strongest. Catch-up continues through age 26 for those who missed the window. Shared decision-making applies for ages 27 to 45.
Age 21 is when Pap screening starts, not vaccination. Waiting until 21 to vaccinate loses the pre-exposure advantage and places it after typical sexual debut in most populations. The two programs run on separate timelines for different reasons.
Age 26 is the catch-up cutoff, not the routine start. Vaccination through 26 is recommended for anyone who missed the 11 to 12 window. For ages 27 to 45, shared decision-making applies. The routine target is still 11 to 12.
Gardasil 9 covers HPV 6, 11, 16, 18, 31, 33, 45, 52, 58. Routine at age 11 to 12 (can start at 9). Catch-up through age 26 (shared decision 27 to 45). Prevents infection; does not clear established dysplasia.
⚠
Do not screen after total hysterectomy for benign disease
If the cervix is gone for benign reasons and no history of CIN2+, no Pap. If hysterectomy was for CIN2+ or cancer, continue vault screening per guidelines. clinical medicine love the "unnecessary Pap after benign hysterectomy" trap.
Prove It
Board Walkthrough
6-vignette bank, 5 dealt per round, answer choices shuffled, never-repeat within a round.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.