Bone is a bank account that quietly drains after menopause. The board game is reading the DEXA number, knowing the one fracture that diagnoses the disease by itself, dosing the bisphosphonate correctly, and ruling out the conditions that steal bone in secret.
The Setup
A Bank Account That Drains
Bone is living tissue under constant renovation. Osteoporosis is what happens when the demolition crew outworks the builders for years, so the scaffolding thins until ordinary stress snaps it.
A 68-year-old woman trips over a rug and lands on her hip from standing height. Imaging shows a femoral neck fracture. Her DEXA done last year reported a T-score of -2.0 at the hip, which falls in the osteopenia range.
What is her bone diagnosis?
Renovation never stops. Throughout life, osteoclasts chew away old bone and osteoblasts lay down new bone. In youth the builders win and you accumulate peak bone mass by your late twenties. After that the balance slowly tips toward resorption, and the question for the rest of life is how fast the account drains.
Estrogen was holding the brakes. Estrogen restrains osteoclasts. At menopause estrogen falls off a cliff → osteoclasts run unchecked → resorption outpaces formation → bone density drops fastest in the first years after menopause. That is why postmenopausal women are the face of primary osteoporosis. The thinning hits trabecular (spongy) bone first, which is why the spine and the femoral neck, rich in trabecular bone, fracture early.
The bone is normal, there is just less of it. This is the key contrast. In osteoporosis the bone that remains is normally mineralized, so the routine labs (calcium, phosphate, alkaline phosphatase, parathyroid hormone) are normal. That normal-lab fingerprint is what separates it from the mimics, where the chemistry is deranged. Flip each card.
OsteoporosisTap to flip
Less bone, normal chemistryReduced bone quantity, normal mineralization. Calcium, phosphate, alkaline phosphatase, and parathyroid hormone are all normal. Diagnosis is by DEXA or a fragility fracture, not by blood tests.
OsteomalaciaTap to flip
Soft, undermineralized boneUsually vitamin D deficiency. Calcium and phosphate run low, alkaline phosphatase and parathyroid hormone run high. Patients have diffuse bone pain and weakness, and films can show Looser zones.
Paget diseaseTap to flip
Chaotic remodelingDisorganized, overactive turnover. The fingerprint is an isolated high alkaline phosphatase with normal calcium and phosphate. Clues include an enlarging hat size, bone pain, and high-output heart strain.
Clinical Images
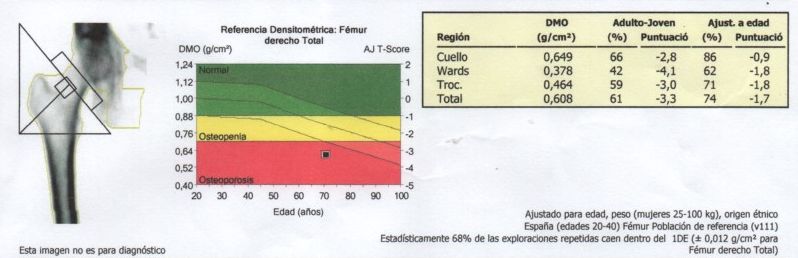
DEXA: measures bone mineral density · tap to expand
Vertebral compression fracture · tap
Where osteoporosis fractures strike · tap
At the Bedside
Silent Until It Snaps
Osteoporosis causes no symptoms until a bone breaks. The exam buys nothing; the history and the fracture pattern do the talking, and a short list of risk factors tells you who is draining fastest.
The disease announces itself with a fracture. The classic three are the vertebral compression fracture (acute back pain or silent height loss and a stooped thoracic curve), the hip fracture (the deadliest, with high one-year mortality in elders), and the distal radius fracture after a fall on an outstretched hand. The defining feature is that the trauma is trivial: a fragility fractureA fracture from a fall at standing height or less, or with no trauma at all. By itself it diagnoses osteoporosis at the hip or spine regardless of the T-score. happens from forces a healthy skeleton would shrug off.
Know the risk factors that drive FRAX. The FRAX tool estimates the 10-year probability of a major fracture and helps decide who with osteopenia still needs drug therapy. Tap each driver.
Older age and female sex
Tap to reveal
The two strongest non-modifiable risks. Risk climbs steeply with each decade, and postmenopausal estrogen loss makes women the dominant group.
Prior fragility fracture
Tap to reveal
The best predictor of the next fracture is a previous one. A single low-trauma vertebral or hip fracture commits the patient to treatment.
Glucocorticoids
Tap to reveal
The most common drug cause of secondary osteoporosis. Chronic steroids suppress osteoblasts and accelerate resorption, so prolonged therapy triggers bone protection on its own.
Tobacco and alcohol
Tap to reveal
Smoking and heavy alcohol both lower bone density and raise fracture and fall risk. These are the modifiable levers worth counseling on every visit.
Low body weight and family history
Tap to reveal
A thin frame means less peak bone mass to spend, and a parental hip fracture signals inherited risk. Both feed directly into the FRAX estimate.
From the Attending
Height loss and a new stooped upper back in an older woman are not just aging. Stacked vertebral compression fractures shorten the spine and bend it forward. Measure height at visits, and when it drops, get spine imaging. A silent vertebral fracture is still a fragility fracture, and it changes the plan.
Reading the Numbers
DEXA, T-Score, and the Secondary Hunt
Three numbers run the diagnosis: the T-score for postmenopausal women, the Z-score for everyone younger, and the FRAX percentage that decides borderline cases. Learn when each applies and the one fracture that overrides them all.
The T-score is a comparison to a young healthy adult. It counts how many standard deviations a patient sits below peak bone mass. -1.0 or above is normal, -1.0 to -2.5 is osteopenia (low bone mass), and -2.5 or lower is osteoporosis. The T-score is the right tool for postmenopausal women and men aged 50 and older.
Work the interpretation. Try each step before you reveal it.
A healthy 67-year-old woman with no fractures has a hip T-score of -2.7. How do you classify her?
A T-score of -2.5 or lower is osteoporosis by densitometry. She qualifies for treatment even without a fracture. T-score at or below -2.5 equals osteoporosis.
A 70-year-old woman with a T-score of -1.8 (osteopenia). Her FRAX shows a 10-year hip fracture probability of 4 percent and major fracture probability of 22 percent. Next step?
FRAX exists exactly for this gray zone. A 10-year hip probability of 3 percent or higher, or a major fracture probability of 20 percent or higher, pushes an osteopenic patient into treatment. Osteopenia plus high FRAX equals treat.
A 34-year-old premenopausal woman is found to have a spine Z-score of -2.6. What does that finding demand?
In a premenopausal woman you use the Z-score, and -2.0 or lower is below the expected range for age. That low a number in someone young means a secondary cause is stealing bone: check for glucocorticoid use, hyperparathyroidism, hyperthyroidism, hypogonadism, celiac disease, or myeloma. Young patient with a low Z-score: find the secondary cause first.
When bone loss looks too aggressive, send the secondary workup. Reasonable first labs include calcium, phosphate, vitamin D, parathyroid hormone, thyroid-stimulating hormone, and a metabolic panel, plus testosterone in men. Tap each secondary cause.
Primary hyperparathyroidismTap to flip
High calcium, high PTHExcess parathyroid hormone pulls calcium out of bone. Look for high calcium with an inappropriately high PTH, often from a parathyroid adenoma. The bone loss is most marked in cortical bone.
HyperthyroidismTap to flip
Fast turnoverThyroid hormone speeds bone remodeling and tips it toward resorption. Suspect it with a suppressed TSH, whether from Graves disease or overreplacement with levothyroxine.
Multiple myelomaTap to flip
Punched-out lesionsConsider it with bone pain, anemia, high calcium, and renal failure. Films show lytic punched-out lesions rather than the diffuse thinning of osteoporosis. Send protein studies.
The Plan
Build the Bone, Dose It Right
Every patient gets the foundation, most get a bisphosphonate, and the board points hide in the dosing rules and the rare-but-tested complications. The anabolic drug and the SERM each have one clean indication or contraindication to memorize.
Foundation for everyone. Adequate calcium and vitamin D, weight-bearing exercise, smoking cessation, limiting alcohol, and fall prevention (vision, home hazards, reviewing sedating medications). These reduce fractures and underpin any drug you add.
Bisphosphonates are first-line. Drugs like alendronate bind bone and poison the osteoclast, slowing resorption so formation can catch up. They cut vertebral and hip fractures and are the default answer for treatment.
Board Trap
The most tested point is how to take an oral bisphosphonate: first thing in the morning on an empty stomach, with a full glass of plain water, then stay upright and take nothing else for at least 30 minutes. Lying down or skipping the water causes pill esophagitis. Rare long-term complications are osteonecrosis of the jaw (often after dental work) and the atypical femoral fracture, heralded by new dull thigh or groin pain.
The other agents each have a niche. Tap each one.
Denosumab
Tap to reveal
A monoclonal antibody against RANKL that shuts down osteoclasts. Useful when kidney function is poor or bisphosphonates fail. Do not stop it abruptly without a follow-on agent, because rebound vertebral fractures can follow.
Teriparatide
Tap to reveal
A parathyroid hormone analog given daily that, pulsed, actually builds new bone (anabolic). Reserved for severe osteoporosis or multiple fractures, limited to about two years. Avoid when osteosarcoma risk is high: prior skeletal radiation, Paget disease, or open growth plates.
Raloxifene
Tap to reveal
A selective estrogen receptor modulator that protects bone and lowers breast cancer risk, a nice fit for a woman who also wants that benefit. The catch is that it raises venous thromboembolism risk and can worsen hot flashes.
Glucocorticoid prophylaxis
Tap to reveal
A patient starting long-term steroids (roughly the equivalent of 7.5 mg of prednisone daily for 3 months or more) should get calcium, vitamin D, and usually a bisphosphonate up front, before bone is lost. Do not wait for a fracture.
Condition
Calcium
Phosphate
Alk phos
PTH
Osteoporosis
Normal
Normal
Normal
Normal
Osteomalacia
Low
Low
High
High
Paget disease
Normal
Normal
High (isolated)
Normal
Primary hyperparathyroidism
High
Low
High or normal
High
From the Attending
Screen the right people: a DEXA for every woman at age 65, every man at 70, and younger postmenopausal women whose FRAX risk is elevated by risk factors. And after any patient over 50 breaks a bone from a minor fall, ask whether it was a fragility fracture. Most of these patients leave the hospital with the broken bone fixed and the osteoporosis never addressed.
Prove It
Board Walkthrough
Seven original clinical vignettes, 5 dealt per round, answer choices shuffled, never repeating within a round. Tap a wrong answer first to see why it almost works, then read the glowing clues.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.