📷 Adrenal mass on scan: localize AFTER biochem · tap to expand
📷 Catecholamine to metanephrine pathway · tap to expand
📷 Pheo: adrenal medulla catecholamine tumor · tap to expand
💉
Pheochromocytoma
The catecholamine bomb in the adrenal medulla. Block the alpha first, or the patient codes on the table.
A 34-year-old woman comes to your clinic for the third time this month. She gets sudden episodes of a pounding headachedrenching sweat and a heart that feels like it's trying to escape her chest. Each spell lasts 15-20 minutes. Her BP today is 198/118. Between episodes she feels totally fine. Routine labs are unremarkable. She's never been on stimulants. Her mother had thyroid cancer at age 40.
What's your top suspicion?
Panic disorder
Graves disease (hyperthyroid)
Pheochromocytoma
Carcinoid syndrome
The Classic Pattern
The Rule of 10s
Tap each card. Front = the rule. Back = why the board cares.
10%
Bilateral
tap
Why it matters
If you find one and miss the other, the BP crisis comes back. Always image both adrenals. Bilateral disease points hard toward familial syndromes (MEN 2, VHL).
10%
Extra-adrenal
tap
Paraganglioma
Same tumor, wrong neighborhood. Most famous spot: organ of Zuckerkandl at the aortic bifurcation. Also head/neck and bladder wall (HTN spike when peeing). MIBG scan finds them.
10%
Malignant
tap
Diagnosis is metastasis
You can't call a pheo "malignant" from histology alone. Malignancy = mets to a non-chromaffin tissue (bone, liver, lung, lymph node). The path slide can't tell you.
10%
In children
tap
Pediatric pheo skews familial
When a kid has pheo, it's genetic until proven otherwise. Higher rate of bilateral, extra-adrenal, and recurrent disease. Screen for MEN 2, VHL, NF1, and SDH mutations.
10%
Familial
tap
Genetic syndromes
MEN 2AMEN 2B (RET), VHLNF1 and SDH mutations (paraganglioma syndromes). Modern data: this number is closer to 25%, but clinical medicine still want 10%.
🧠Memory hook: "Ten Bilateral Extras Made Children Familial."🔑10% Bilateral, 10% Extra-adrenal, 10% Malignant, 10% Children, 10% Familial. Stupid sentence, sticks like glue.
Why the symptoms hit the way they do
Headache: the catecholamine spike yanks BP up → cerebral vessels stretch → pounding pain.
Sweating: sympathetic outflow hits sweat glands directly. No fever, just soaked.
Palpitations: beta-1 receptors on the heart get hammered → rate and force both jump.
Hypertension: alpha-1 on vessels clamps everything down. Either paroxysmal spikes or sustained baseline-high.
Pallor + cold extremities: alpha-1 vasoconstriction. Pheo patients blanch they don't flush. That's how you separate it from carcinoid.
⚠
Pheo vs Carcinoid, different mediators, opposite skin
Pheo dumps catecholamines (alpha-1 = vasoconstriction = pale). Carcinoid dumps serotonin & bradykinin (vasodilation = flushing + diarrhea + wheezing). Both make HR jump. Only one turns the patient red.
Workup
Diagnose, Then Image
Biochemistry first. Imaging only after the labs say so.
Plasma free metanephrines
Best screening test, highest sensitivity. Catch the easy positives.
Why: metanephrines are the breakdown product. Tumors leak constantly even between BP spikes, so the metabolite stays elevated.
24-hour urine metanephrines + catecholamines
Best confirmatory test, highest specificity. This is the answer when the clinical medicine ask "most specific."
Why: 24 hours captures the whole day, including a paroxysm. Spot catecholamines miss the spell.
CT or MRI of the adrenals
Localize the tumor after labs are positive. Never image first.
Why: imaging an asymptomatic adrenal nodule with no biochem support → you find the 4% incidentaloma, not the pheo.
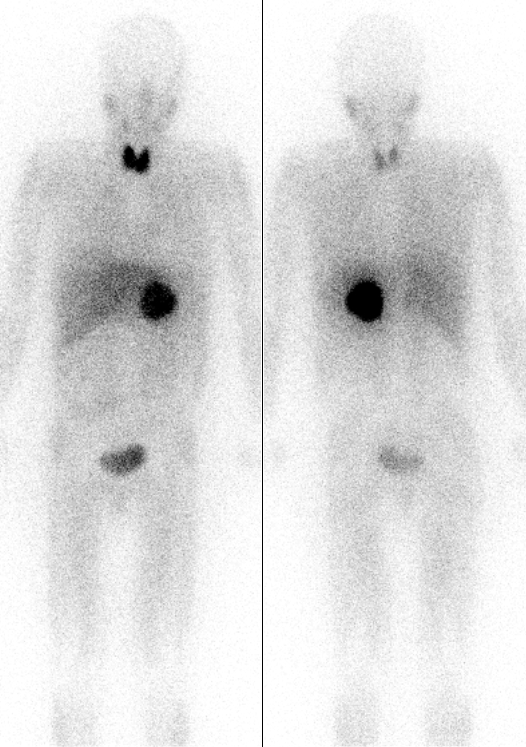
MIBG scan
For extra-adrenal, multifocal, or metastatic disease. MIBG (a norepi analog) lights up chromaffin tissue anywhere.
Why: a CT can't scan the whole body for paraganglioma. MIBG can.
⚠
Normal catecholamines do NOT rule it out
Pheo secretes paroxysmally. A spot serum draw between episodes can read normal. That's why we screen with metanephrines (the metabolite, always elevated) and confirm with the 24-hour urine (catches the spell).
The Treatment Trap
Order Matters. Get It Wrong, You Kill Them.
Click the steps in the correct order. Beta-block first and the patient codes.
Treatment Sequence
Drag (well, tap) the steps into slots 1, 2, 3 in the correct order. Pre-op pheo management.
STEP 1
empty
STEP 2
empty
STEP 3
empty
Why α before β? The mechanism that actually sticks.
Catecholamines hit two main vascular receptors:
α-1 on blood vessels → squeezes them shut (vasoconstriction, HTN).
β-2 on blood vessels → relaxes them (vasodilation, mild offset).
The pheo's catecholamines are pushing on both at once. The β-2 dilation is a tiny pressure-release valve.
If you give a non-selective β-blocker first you slam the β-2 release valve shut while α-1 is still wide open and hammering. Result: unopposed alpha vasoconstriction → severe hypertensive crisis → stroke or MI on the table.
So: α-block first with phenoxybenzamineNon-selective, irreversible α-blocker. "Irreversible" matters: even when the tumor dumps a fresh load of catecholamines mid-surgery, the receptors are already permanently blocked. The protection doesn't wear off. for 10-14 days. Then add a β-blocker for the reflex tachycardia. Then operate.🔑Alphabet rule: A before B. Never B before A.
💍Perioperative care: aggressive IV hydration (the chronic vasoconstriction has shrunk their plasma volume), continued α-blockade, BP monitoring through the case, and prep for post-op hypotension once the tumor is yanked out.
See It Happen
The Receptor Pressure Stage
Watch the vessel. Pick a blockade strategy and see what the lumen does in real time.
Vessel Lumen Simulator
The tumor floods both α-1 (clamps vessels shut) and β-2 (the small vasodilation release valve). The order you block them decides whether the lumen opens or slams shut.
BP 198/118 · lumen clamped
Baseline pheo: catecholamines hammer α-1, vessels are squeezed nearly shut, pressure is sky-high.
Reason It Out
Workup Decision Tree
Commit to an answer first. Each step reveals the consequence only after you choose.
A 34-year-old woman has episodic headache, palpitations, and diaphoresis with a spell BP of 198/118; between spells she is normotensive. What is the single best FIRST move?
Biochemistry before imaging. Plasma free metanephrines have the highest sensitivity and stay elevated between paroxysms. Image only after the labs are positive, or you chase a 4% incidentaloma. And never start a beta-blocker before alpha. Break it down: confirm with metanephrines, then localize.
Metanephrines come back 8x normal and CT shows a 4 cm right adrenal mass. Surgery is in 2 weeks. Which drug is started FIRST?
Alpha first, always. Phenoxybenzamine is an irreversible alpha-blocker: block α-1 for 10 to 14 days so the vessels open and plasma volume expands. Beta first slams the β-2 release valve shut against wide-open α-1 = unopposed alpha = crisis. Break it down: phenoxybenzamine first, beta second, knife last.
After 12 days of phenoxybenzamine the BP is 128/76 but resting heart rate is now 118. What is the next step before the OR?
Now beta is safe. The reflex tachycardia appears once vessels dilate; because α is already covered, adding propranolol is correct and the alpha stays on through induction. A thiazide is the wrong direction in a volume-depleted pheo patient. Break it down: beta is fine, but only after alpha.
The Genetic Crowd
MEN 2A vs 2B vs VHL
Pheo doesn't travel alone. Know the company it keeps.
MEN 2A
RET mutation
Pheochromocytoma
Medullary thyroid cancer (calcitonin)
Parathyroid hyperplasia (chief cells)
3 Ps of MEN 2A: Pheo, Parathyroid, Papillary… wait, no. Medullary thyroid. Adjust.
MEN 2B
RET mutation
Pheochromocytoma
Medullary thyroid cancer
Marfanoid body habitus
Mucosal neuromas (lips, tongue, GI)
NO parathyroid involvement
Tall, lanky kid with bumpy lips and a tongue full of nodules → MEN 2B until proven otherwise.
🧠2A vs 2B mnemonic: 2A = Adenomas (parathyroid). 2B = Bumps (mucosal neuromas) and Body (Marfanoid). Same RET gene, different downstream.
🕱
Pheo in pregnancy
High maternal and fetal mortality if missed. Catecholamine surge during labor can crash both. Hypertension in pregnancy that isn't preeclampsia (no proteinuria, episodic, with sweating/palpitations) deserves a metanephrine check. Phenoxybenzamine pre-delivery, C-section preferred, surgery after.
3 of 4
The Patient
Episodic HTN, Sweating, Headache
A 34-year-old woman walks in. Pick the diagnosis from the story.
🎯The 3 Ps nail it: Pressure + Perspiration + Palpitations in episodic spells. Mom with medullary thyroid cancer is the second clue, think MEN 2A.🔑Pheo = the 3 Ps. Pressure, Perspiration, Palpitations. If only 1 or 2 show up, you're still in the differential.
What is pheochromocytoma actually doing?
It's a tumor of the chromaffin cellsChromaffin cells live in the adrenal medulla. They're basically modified sympathetic neurons, they pump out epi/norepi when the sympathetic nervous system fires. in the adrenal medulla. Those cells normally release epinephrine and norepinephrine when your sympathetic nervous system fires. The tumor releases them on its own in unpredictable bursts.
That's why the symptoms are paroxysmal the tumor dumps catecholamines, the patient spikes, the catecholamines wash out, the patient feels normal. Repeat.
Some pheos also pump out dopamine. Extra-adrenal versions (paragangliomas) often secrete only norepi.
1 of 4
The Syndromic Zoo
The Lineup
Seven villains. Pheo is just the start. Tap each card to flip.
💥
Pheo
Adrenal medulla catecholamine bomb. Rule of 10s.
Pheochromocytoma
Origin: adrenal medulla chromaffin cells
Rule of 10s: 10% bilateral, 10% extra-adrenal, 10% malignant, 10% in kids
Step 1: Biochemical screening.
Order: plasma free metanephrines (best sensitivity, can be drawn any time)
OR 24-hour urine metanephrines (high specificity, good confirmation).
Do NOT image first. Imaging without biochem confirmation finds incidentalomas and confuses the workup.
Still screen biochemically.
Pheo can present with sustained (not just episodic) HTN, especially in familial cases. If index of suspicion exists (family history, young patient, resistant HTN), order plasma metanephrines before dismissing it.
Biochemical screen result?
Step 2: Anatomic localization.
CT or MRI of the adrenals. CT preferred for adrenal (sensitivity ~90%). MRI preferred if: pregnancy, allergy to contrast, or suspected extra-adrenal tumor.
If CT is negative but biochem is strongly positive: whole-body MIBG scan or PET to find extra-adrenal paraganglioma.
Pheo unlikely, but:
If suspicion remains high (paroxysmal spells, family history), repeat testing during a symptomatic episode. Catecholamines have a short half-life; a random draw between spells can be falsely negative. Metanephrines are more stable but can occasionally miss low-secretors.
Tumor found on imaging. Pre-op management?
Correct sequence.
Phenoxybenzamine (non-selective irreversible alpha-blocker) for 10-14 days minimum.
Goals: normalize BP, relieve vasoconstriction, allow plasma volume to expand.
Expect reflex tachycardia once vessels dilate. Then add beta-blocker (propranolol) AFTER alpha is established. Never beta-block first = unopposed alpha = hypertensive crisis on the table.
Dangerous.
Surgical manipulation of a pheo releases massive catecholamines. Without pre-op alpha-blockade, intraoperative HTN crisis, arrhythmia, and death are likely.
The pre-op alpha-blockade period is non-negotiable. Minimum 10-14 days. Some centers use 4-6 weeks.
After adequate alpha-blockade (BP controlled, 10-14 days)?
Correct final sequence.
Once alpha is covered and BP is stable: add propranolol to control reflex tachycardia.
Then: laparoscopic adrenalectomy (preferred for tumors <6cm).
Post-op: watch for hypoglycemia (catecholamine withdrawal drops counter-regulatory hormones) and hypotension (vasodilation now unopposed by tumor).
Prove It
Board Walkthrough
25-vignette bank, 5 dealt per round, answer choices shuffled, never-repeat within a round. Tap a wrong answer first to see why it almost works, then read the glowing clues.
4 of 4
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.