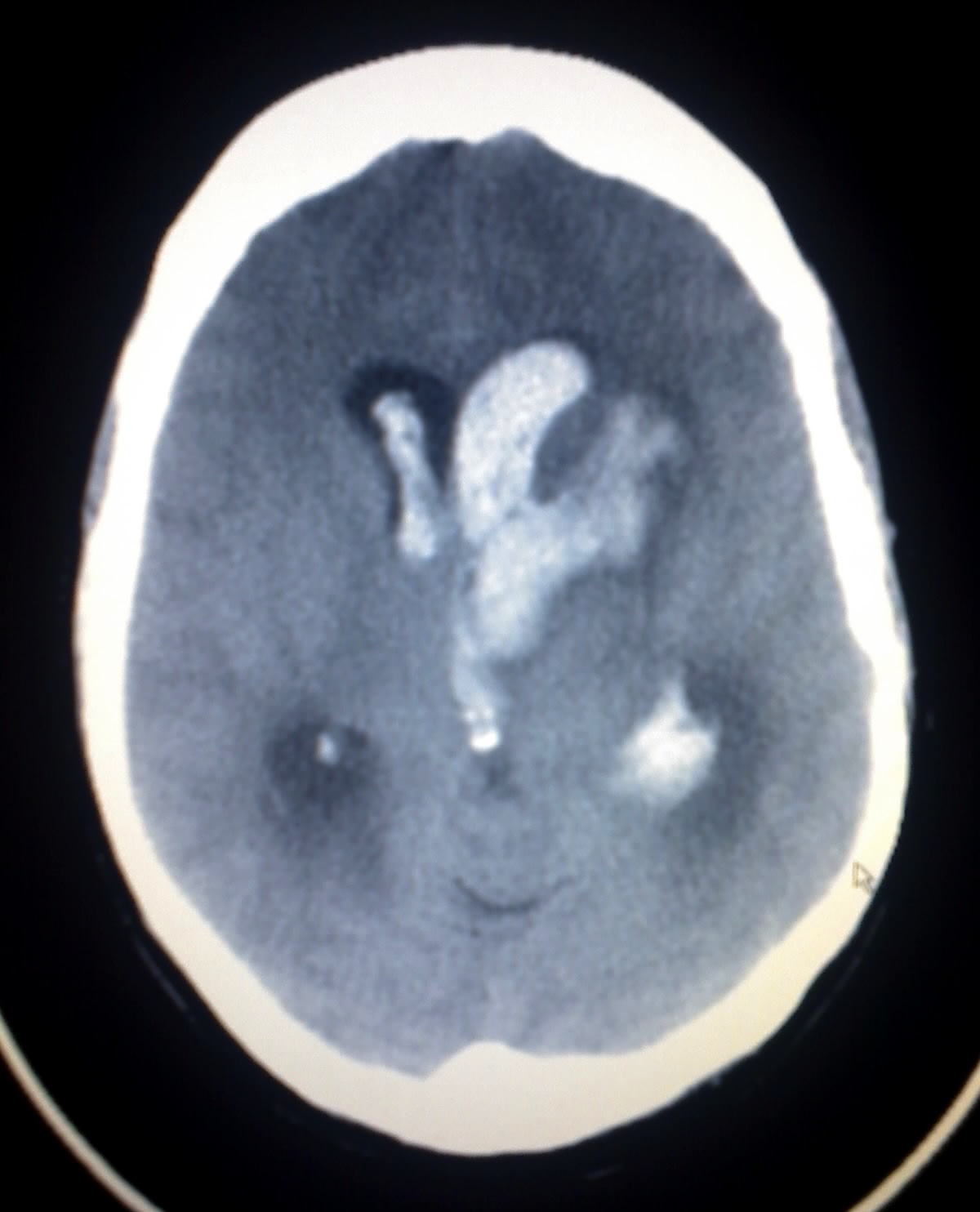
Intraparenchymal hemorrhage · Hypertensive microaneurysm · Deep brain vessels
Read the case. Choose before you scroll. The clues are already there.
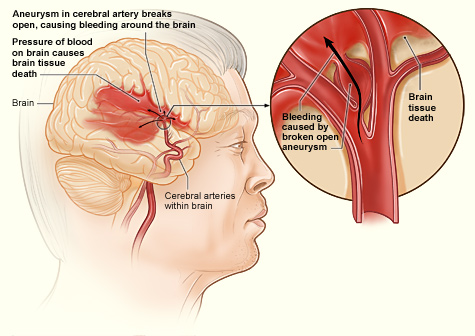
Watch hypertension destroy a deep penetrating artery one stage at a time. Advance through the chain.
Every hemorrhage has a signature. Lock in the discriminators.
Work through the CT findings step by step. Choose at each node before the feedback appears.
Tap each card to reveal the hook.
Tap any image for the full view.