Five dysfunctions of the sphenobasilar synchondrosis: two physiologic, three traumatic. Know the axes, the naming rules, and which ones can happen normally.
A 27-year-old recreational soccer player has frontal headaches and neck pain that began after a ball struck the left side of her head. Vault-hold palpation feels like a skewed parallelogram: the examiner's index fingers drift right, while the little fingers drift left. Which SBS strain pattern is present?
Toggle between flexion and extension to see what every structure does in each phase.
The sphenobasilar synchondrosis moves superiorly. Picture pushing up on a rubber ball from below: it squishes wider and shorter. That is cranial flexion.
Temporal and parietal bones rotate outward, spreading the vault. When the ball squishes wider, the sides flare out. Same thing.
As it widens transversely, the front-to-back distance shrinks. The ball gets fatter but shorter. Wider + shorter = flexion.
The sacral base tips posteriorly (counternutation = sacral flexion). The sacrum rocks back as the cranium widens. They are coupled through the dural tube.
The SBS descends inferiorly. Now let go of the ball: it springs back to tall and narrow. The skull narrows transversely and lengthens AP. Opposite of flexion.
Temporal and parietal bones rotate inward. The sides pull back in as the vault narrows. Everything tightens and lengthens.
As the skull narrows, the AP distance increases. Narrower + longer = extension. The skull stretches out front-to-back.
Sacral base tips anteriorly (nutation = sacral extension). S in Spine: the spine straightens as the sacrum nutates. Extension phase tightens and lengthens everything.
CRI is the palpable rhythm of the PRM. Slower than respiration, faster than heart rate variability.

Toggle between extension and flexion. Watch the SBS, spinal cord, and sacrum move together.
Tap each tab. Know the naming rule, the axis, and whether it is physiologic or traumatic.
Pick a strain pattern and watch the same vault-hold contacts move. Index contacts ride the sphenoid greater wings. Little-finger contacts ride the occiput. The board trick is deciding which contact actually names the pattern.
Index contacts drift right while little-finger contacts drift left. That side-to-side parallelogram is the lateral strain pattern.
The sphenoid and occiput rotate around the anteroposterior (AP) axis in OPPOSITE directions. One greater wing goes up, the other goes down.
Naming: Named for the HIGH greater wing of the sphenoid. If the left wing is superior, it is a left torsion.
Example: Left torsion = left greater wing superior, right greater wing inferior. The sphenoid and occiput are twisting around the AP axis like wringing a towel.
Classification: Physiologic. Can occur during normal cranial motion. No trauma required.
The sphenoid and occiput sidebend in the SAME direction but rotate around vertical axes in OPPOSITE directions. This creates a convexity on one side of the SBS.
Naming: Named for the convexity (the sidebend direction). If the SBS is convex to the left, it is a left SB-R.
Example: Left SB-R = SBS convex to the left. Both bones sidebend left (same direction), but they rotate around their vertical axes in opposite directions.
Classification: Physiologic. Can occur during normal cranial motion.
This is the part the boards love. Vertical strains move on TWO parallel transverse axes, and the sphenoid and occiput rock the same rotary direction around them. Their tops tip the same way, not the mirror-image way of normal flexion.
Because flexion and extension are named in mirror image for the two bones, that one motion reads as one bone flexed and the other extended. That is why the notation is SFOE or SEFO and never both-flexed. The net result is the sphenoid base riding superior or inferior relative to the occiput.
Naming: Named for the sphenoid, and the notation spells out what BOTH bones are doing in two letters each.
Superior vertical strain (SFOE): Sphenoid Flexed, Occiput Extended. The sphenoid base rides superior. Classic cause: an anterior central blow to the frontal bone driving the sphenoid base up.
Inferior vertical strain (SEFO): Sphenoid Extended, Occiput Flexed. The sphenoid base rides inferior. Trauma can come from anterior or posterior to the SBS.
Classification: Non-physiologic. Always a trauma finding.
The sphenoid and occiput translate laterally in opposite directions around two parallel vertical axes. This is a shear: one bone slides left while the other slides right.
Naming: Named for the side the sphenoid (basisphenoid) translates toward relative to the basiocciput. If the sphenoid shifts left, it is a left lateral strain. Read the SPHENOID direction, never the occiput.
Mechanism: Most commonly from birth trauma, also a lateral blow to the head. The sphenoid and occiput slide past each other like tectonic plates.
Classic sign in children: a "parallelogram head" with facial asymmetry. The skew of the basisphenoid against the basiocciput skews the whole face.
Symptoms: may cause headache and visual disturbances.
Classification: Non-physiologic. Requires trauma.
The SBS is jammed together. No flexion or extension can occur at the synchondrosis. The cranial mechanism is essentially locked.
Naming: Just "compression." No left or right, no superior or inferior. The joint is stuck.
Mechanism: Most commonly from birth trauma (difficult delivery, forceps). Can also result from severe head trauma at any age.
Clinical: The CRI will be diminished or absent on palpation. The cranium feels rigid, with no inherent motion at the SBS.
Classification: Non-physiologic. Always trauma.
Where the sutures meet. Tap each card for the bones that converge, the old fontanelle, and the board trap underneath.

Junction of the greater wing of the sphenoid, the temporal, the parietal, and the frontal bones. The sutures form an H shape. Located just behind and above the zygomatic arch (roughly at the temple).
Why it is dangerousThe middle meningeal artery runs deep to the pterion. A fracture here can tear the artery and produce an epidural hematoma, the classic lucid-interval bleed. The pterion is the thinnest part of the lateral skull.
Board trapLateral head trauma plus "talk and die" lucid interval points to pterion fracture and middle meningeal artery, NOT a bridging vein (that is the subdural at a different site).
 Red box marks the pterion on a real skull: the H where four bones meet at the temple.
Red box marks the pterion on a real skull: the H where four bones meet at the temple.
Junction of the occipital, temporal, and parietal bones. It is where the occipitomastoid, parietomastoid, and lambdoidal sutures come together.
LocationSits just behind the ear. A surgical landmark for the posterolateral skull and the transverse-sigmoid sinus junction underneath.
Board trapDo not confuse with pterion. Pterion is anterior (temple, four bones, H, middle meningeal artery). Asterion is posterior (behind the ear, three bones, three sutures).
 Red box marks the asterion behind the ear: occipital, parietal, and temporal bones.
Red box marks the asterion behind the ear: occipital, parietal, and temporal bones.
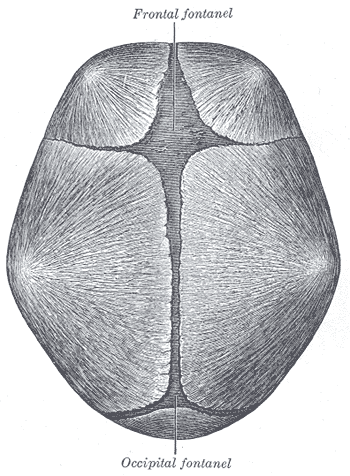
Junction of the sagittal suture, the coronal suture, and the metopic (frontal) suture. Sits at the top of the vault in the midline.
Was a fontanelleThis was the anterior fontanelle, the largest one. It closes by roughly 18 to 24 months. A bulging anterior fontanelle in an infant signals increased intracranial pressure.
Board trapAnterior fontanelle needs THREE sutures: sagittal plus coronal plus metopic. Leaving out the metopic suture is the classic half-right miss.
 Bregma boxed at the top of the vault (coronal meets sagittal); pterion, asterion, and lambda shown for context.
Bregma boxed at the top of the vault (coronal meets sagittal); pterion, asterion, and lambda shown for context.
Junction of the sagittal suture and the lambdoid suture, at the back of the vault in the midline. Named for its resemblance to the Greek letter lambda.
Was a fontanelleThis was the posterior fontanelle. It closes early, by about 2 to 3 months, much sooner than the anterior fontanelle.
Board trapSagittal plus lambdoid is the POSTERIOR fontanelle at lambda. Sagittal plus coronal plus metopic is the ANTERIOR fontanelle at bregma. Mixing the two is the most common suture error.