Osteopathic Manipulative Medicine · Respiratory-Circulatory Model
Lymphatics Open the Pathway, Then Move the Fluid
Two ducts, one drain, four pumps, and a contraindication list the clinical medicine adore. Everyone overthinks lymph. The whole topic is a plumbing problem. Start with the question that catches most students.
Medically reviewed by Fatima Ali, DO & Kaitlyn Cocuzzo, MD✦elite
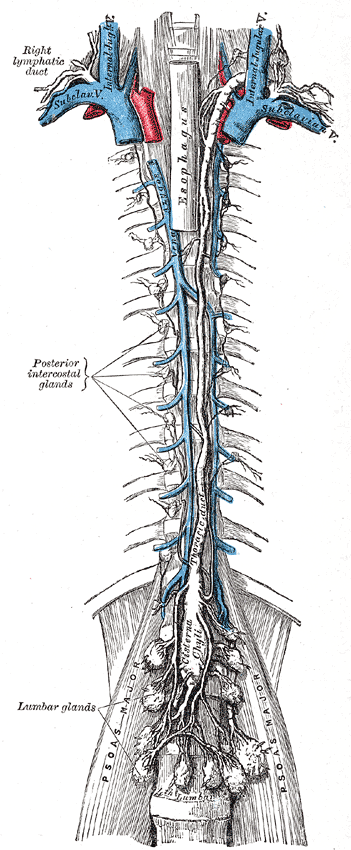
The lymphatic drainage system: green vessels collect fluid from tissues and route it through node chains back to the venous system at the subclavian-IJ junction.
Before you scroll
A 61-year-old man is brought to the office because of progressive swelling of his face and both legs over 3 weeks. Examination shows puffiness of the head and neck, the left chest wall, and both lower extremities, while the right arm and right side of the head are spared. A chest radiograph shows a posterior mediastinal mass. Which single structure, if obstructed, best explains this exact distribution of swelling?
What does the thoracic duct actually drain?
Both legs, the abdomen and pelvis, the left chest, the left arm, and the left head and neck: about 75 percent of the body. That matches the swelling exactly.
Why is the RIGHT arm and right head spared?
The right upper quadrant above the diaphragm drains the OTHER way, through the right lymphatic duct. A thoracic-duct block cannot back up territory it never carried.
Put it together.
Both legs + left chest + spared right arm = thoracic duct obstruction, here from a mediastinal mass compressing the duct. Both ducts ultimately empty near the right atrium, so a duct lesion swells exactly its own territory.
Scroll ↓ the two ducts come next
The Plumbing
Drag the Body to Its Duct
There are only two terminal pipes. The right lymphatic duct takes the right upper quadrant; the thoracic duct takes everything else. Drag each body territory into its duct. The pattern is the whole anatomy question.
The lymphatic system: a network of vessels and nodes that collects leaked fluid and returns it to the blood via two terminal ducts.
Right Lymphatic Duct
drains into right subclavian / IJ junction
Thoracic Duct
begins at cisterna chyli (L1), empties left subclavian / IJ junction
Right head & neckRight armRight thoraxLeft head & neckLeft armLeft thoraxBoth legsAbdomen & pelvis
Drag (or tap a chip below, then a duct) to sort each territory. Get all 8 to unlock the takeaway.
The takeaway you carry to the exam
Right upper quadrant above the diaphragm → right lymphatic duct. Everything else (~75%) → thoracic duct.
So the swollen body part tells you the blocked pipe. Right arm + right face only? Right lymphatic duct. Both legs + left chest? Thoracic duct. Heart and lungs themselves drain to the right supraclavicular fascia (right duct); the "fascia of the thoracic duct" is a LEFT-sided structure and does not drain the heart.
RIGHT duct = the small one, just the Right Upper corner. Thoracic = the big 75% pipe for everyone else.
The Route
The Thoracic Duct's Run
One pipe, three landmarks the clinical medicine test: where it starts, where it crosses the diaphragm, and where it ends. Tap each landmark.
The thoracic duct (blue) starts at the cisterna chyli near L1, climbs alongside the aorta through the posterior mediastinum, and empties at the left subclavian-IJ junction.
Tap a landmark to trace the route and see why it matters.
Starts low at the cisterna chyli (L1), sneaks through the spine at the aortic hiatus (T12), climbs, and dumps at the LEFT venous angle. Everyone meets near the right atrium in the end.
The Edema Engine
Two Reasons Fluid Leaves a Vessel
Lymph is just the fluid that leaked out and has to be carried home. There are only two ways to force it out, plus a way the leftover gets stuck. Flip each switch and watch the leak.
→←
capillary
interstitial tissue
lymph drain: open
1 · Hydrostatic pressure (push, e.g. heart failure)
2 · Oncotic (protein) pull, e.g. nephrotic / cirrhosis
3 · Lymphatic drainage (the cleanup pipe)
All three normal: the little bit that leaks gets carried home by lymphatics. No swelling.
The whole edema rule in one line
Fluid leaves the vessel for only two reasons: too much push (high hydrostatic) or too little pull (low oncotic).
Lymphatics normally mop up the leak AND the leaked protein and return both to the blood. Block the lymphatics and protein piles up in the tissue, which is the third edema mechanism. That protein is why the swelling turns firm and non-pitting.
Tap to reveal the pitting rule
Watery + low protein (heart failure, nephrotic) = PITS. Protein-rich (lymph block, filariasis, post-mastectomy) = NON-pitting, and it grabs the toes (Stemmer sign). Protein holds its shape; water runs away from your thumb.
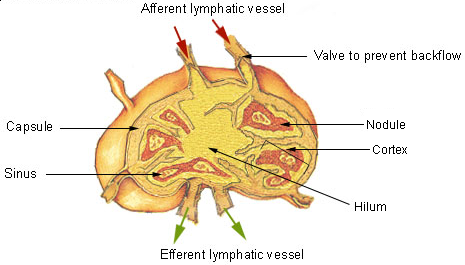
Cross-section of an aggregated lymphatic nodule. Lymphocytes cluster in follicles around germinal centers where B cells mature and mount immune responses.
The OMM hook nobody expects
Lymphatic vessels are adrenergic: sympathetics SQUEEZE them shut.
The thoracic duct and terminal lymphatics carry sympathetic (adrenergic) nerves and no reliable parasympathetics. High sympathetic tone constricts the big terminal vessels and chokes flow. That is why OMM treats the facilitated segments (rib raising) to decompress the lymphatics: less sympathetic squeeze means a wider lumen and more flow.
Sympathetics = a hand on the hose. Calm them and the lymph runs.
Tap to reveal the gut-fat hook
Lacteals are the gut's lymphatics, and they carry FAT. Long-chain fats get packaged into chylomicrons, enter lacteals, become chyle, and drain through the thoracic duct as milky lymph. Medium-chain fats skip lacteals and ride albumin straight to the portal vein. Separate drug hook: ezetimibe does not block lacteals. It blocks NPC1L1 at the intestinal brush border, lowering cholesterol absorption.
Open the Pathway, Then Move the Fluid
Build the Treatment Sequence
If you pump before you open the drain, fluid backs up against a closed door. Drag the four steps into the order that actually works. This order is the single most tested OMM rule on this topic.
The diaphragm: a muscular dome between the thorax and abdomen. On inhalation it descends, creating negative thoracic pressure that sucks lymph upward through the thoracic duct.
Drag (or tap a step, then a slot) to build the order. Fill all four to lock it in.
Why this exact order
1. Thoracic inlet first ("break the dam"). Both ducts pass through Sibson's fascia at the thoracic inlet. A restriction here can swell the WHOLE body because both pipes are pinched. Open it or everything you pump just backs up.
2. Dome the diaphragm. The diaphragm is the engine of the two-chambered pump: on inhalation, negative chest pressure + positive belly pressure suck lymph upward. Restore that excursion and lymph moves with every breath.
3. Pumps. NOW you actively promote flow: Miller thoracic pump, pedal pump, and friends.
4. Chapman points last. Only after the pelvis and leg lengths are balanced.
Open the door, start the engine, pump the fluid, Chapman last. Pump-before-open is the trap.
Know Which Pump, And When NOT To
The Named Pumps
Each pump has a signature setup, a signature indication, and a signature trap. Tap a tab. The contraindication line is the one the clinical medicine actually test.
Lung-specific lymphatic pump
Miller Thoracic Pump
Technique image
Hands on the anterior chest. The force is rhythmic chest compression, then release. This is the lung-congestion pump after the inlet is open.
Setup
Supine, hands on anterior chest wall
Dose
Rhythmic compress / release ~2 cycles/sec, several breaths
Metastatic cancer (can seed tumor via lymphatics); rib/spinal fracture; lymphatic-system malignancy; osteoporosis (relative)
After you open the thoracic inlet, the Miller pump is the lung's lymphatic technique. The board trap: a patient with metastatic cancer who has a cough. Do NOT pump.
Whole-body lymphatic pump
Pedal Pump (Dalrymple)
Technique image
Contact is at the feet. The force is rhythmic dorsiflexion and release, sending a wave through the legs and trunk.
Setup
Supine, operator at the feet
Dose
Rhythmic dorsiflexion / oscillation
Indication
General whole-body lymphatic congestion, lower-extremity edema, fluid return
Contraindication
Osteonecrosis / acute fracture / dislocation in the limb; unstable cardiac condition; moderate-to-severe CHF
The general pump that moves everything. Trap: a great-toe osteonecrosis under your contact, or a patient in decompensated heart failure.
Massages the cisterna chyli
Abdominal Pump
Technique image
Hands over the upper abdomen. The force is gentle compression with respiration, aimed at the cisterna chyli/thoracic duct origin near L1.
Setup
Hands on the abdomen, follow respiration
Dose
Rhythmic compression, paced to breathing
Indication
GI dysfunction, CHF, COPD/asthma, URI; directly massages the thoracic duct at the cisterna chyli
Contraindication
Rib/spinal fracture; traumatic disruption of liver or spleen; full stomach; nearby surgical incision; lymphatic malignancy
It squeezes the cisterna chyli, the thoracic duct's reservoir at L1. Trap: it can aggravate GERD, so use care in reflux.
ENT / mandibular drainage
Galbreath Technique
Technique image
Contact is the mandible. The force is gentle traction along the jaw to help Eustachian tube and middle-ear drainage.
Setup
Supine, head turned, gentle mandibular drainage
Dose
Gentle traction, part of the ENT sequence
Indication
Recurrent otitis media, Eustachian/middle-ear and sinus drainage, URI
Contraindication
Recent mandibular fracture
Mandible drainage for the stuffy middle ear. The single trap: a recent mandibular fracture.
Upper-extremity / chest mobility
Pectoral Traction
Technique image
Contact is the anterior axillary folds. The force is sustained lateral traction while the patient breathes.
Setup
Operator at the head, grips the anterior axillary folds
Standard spinal precautions (acute fracture, instability)
The autonomic move: it calms sympathetics, which decompresses the adrenergic terminal lymphatics and lets the terminal vessels open.
Board Gold · The Do-Not List
Who Do You NOT Treat?
Each round shows one technique and four patients. Tap the patients you must NOT treat. Two of every three lymphatic questions on the clinical medicine live right here.
The unifying theme
The universal "do not pump": malignancy, fracture / osteonecrosis / acute trauma at the contact, and unstable cardiac / moderate-severe CHF for whole-body pumps.
Add the specific ones: doming the diaphragm is out with a full stomach or an AAA / pulsatile mass (rupture risk: image first), but it is FINE in pregnancy. Galbreath is out with a recent mandibular fracture. Cervical chain drainage is relatively contraindicated with carotid disease, tender reactive nodes, or bradyarrhythmia.
Cancer, broken bone, crashing heart. Plus: full stomach or AAA stops the diaphragm (not pregnancy).
When Lymph Goes Wrong
The Lymph Villains
Four board-favorite pathologies. Use the arrows or tap a card to open one file at a time.
Stage-3 lymphedema (firm, non-pitting, toes involved)Elephantiasis (filariasis, Wuchereria)Lymphangitis (the red streak)Ascending red line along a lymphaticLymphatic vessels & thoracic ductLymphatic system overview
Inside a lymph node: the outer cortex holds B-cell follicles, the paracortex holds T cells, and lymph filters through sinuses before exiting via the efferent vessel.
1 / 4 · Lymphedema
🦵
Lymphedema
protein-rich, non-pitting, toes involved
▼
Look
Firm, non-pitting swelling that grabs the toes · positive Stemmer sign (cannot tent the skin over the second toe).
Primary
Inherited / congenital (Milroy, and Turner syndrome). Turner chain: failed fetal lymph drainage → cystic hygroma, a fluid-filled neck lymph sac → webbed neck plus newborn non-pitting hand and foot edema.
Secondary
Acquired: post-mastectomy with axillary node dissection, radiation, or filarial infection (Wuchereria) causing elephantiasis.
Late trap
Chronic post-mastectomy lymphedema can spawn a cutaneous angiosarcoma (Stewart-Treves syndrome).
vs CVI
Venous insufficiency PITS, improves overnight, spares toes, and stains the medial ankle. Lymphedema is firm, persistent, toes-in.
➡
Lymphangitis
the red streak racing up a limb
▼
Look
A flat red area with a red line / streak tracking proximally: the bacteria are crawling UP the lymphatic channel, inflaming it as they go.
Bug
Group A Strep (S. pyogenes). Mnemonic LINES: Lymphangitis, Impetigo, Necrotizing fasciitis, Erysipelas, Scarlet fever.
Why Strep
Strep must follow channels, so it makes a line. Staph uses enzymes to eat sideways through tissue, so it spreads in a circle (cellulitis), not a line.
Nodular variant
An ascending NODULAR lymphangitis after a thorn prick = Sporothrix (the rose gardener), treat with itraconazole.
A lymph node chain: fluid enters through afferent vessels, filters through the node, and exits via efferent vessels. Nodes swell when they trap infection or cancer cells.
👑
Lymphadenopathy: red-flag nodes
which node location changes the urgency
▼
Highest risk
Supraclavicular nodes are the strongest malignancy red flag. Left supraclavicular = Virchow node from abdominal/GI cancer until proven otherwise.
Elbow node
Epitrochlear node, not nerve. It sits near the medial elbow and drains the ulnar forearm/hand. Palpable is abnormal; if there is no local infection or systemic cause, persistent enlargement needs workup/biopsy.
Groin trap
Inguinal nodes are often reactive from leg/genital drainage and have lower biopsy yield. Biopsy only when suspicious: hard, fixed, very large, persistent, or paired with systemic cancer signs.
Elsewhere
Most tender/mobile nodes are infection (often viral). Watch briefly if the story is benign and it is shrinking; escalate if it persists, grows, hardens, or comes with fever, night sweats, or weight loss.
Special nodes
Sister Mary Joseph node (periumbilical) = intra-abdominal cancer. Testes/ovaries drain to para-aortic nodes, not inguinal.
Spread rule
Carcinomas spread by lymphatics; sarcomas spread by blood (CLaSH). The sentinel node is the first node draining a tumor (breast = axillary).
🥛
Chylothorax
milky pleural fluid from a duct injury
▼
Look
Milky, triglyceride-rich pleural fluid · it is an EXUDATE.
Cause
Rupture or obstruction of the thoracic duct: trauma, surgery, or malignancy (classically lymphoma).
Buzz case
A teen with an abdominal mass just left of the umbilicus + chylous effusion + "starry sky" biopsy = Burkitt lymphoma invading the duct/cisterna chyli.
Board reflex
"Disruption of the thoracic lymphatic duct" on a pleural effusion question = think cancer.
Build the Diagnosis
Read the Swelling
A real case, one decision at a time. Guess each branch before it opens. The tree is the algorithm you run on test day.
Don't Kill The Patient
Five Quick Calls
Five rapid questions pulled from a bigger pool, reshuffled every visit. Cross out (right-click / long-press) and highlight (select text) as you read.
clinical Practice
Walk the Cases
Full clinical vignettes, one at a time, in a shuffled order. Progress saves to your account on this device. Cross out (right-click / long-press) and highlight (select text) as you go.
Tip: kill the wrong choices first, then read the explanation chain for every option.
Reviewed by Fatima Ali DO and Kaitlyn Cocuzzo MD. Practice cases use rebuilt demographics, values, and answer order.
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.
Free preview complete
This is where Elite starts
The full board walkthroughs, elimination drills, and deeper mechanics are inside Elite.
Unlock every gated Bone Wizardry page
Keep the one-at-a-time walkthrough banks
Use the diagnostic games and answer logic without limits